

Usefulness of an intraoperative flipped monitor in laparoscopic surgery with situs inversus totalis: a case report of laparoscopic-assisted ileocecal resection
- PMID: 38190089
- PMCID: PMC10774461
- DOI: 10.1186/s40792-023-01806-5
Usefulness of an intraoperative flipped monitor in laparoscopic surgery with situs inversus totalis: a case report of laparoscopic-assisted ileocecal resection
Abstract
Background: Situs inversus totalis (SIT) is a rare congenital condition that involves complete transposition (right to left reversal) of the visceral organs. Laparoscopic surgery can be challenging because of the mirror-image anatomy. We describe a surgical innovation in laparoscopic surgery for SIT.
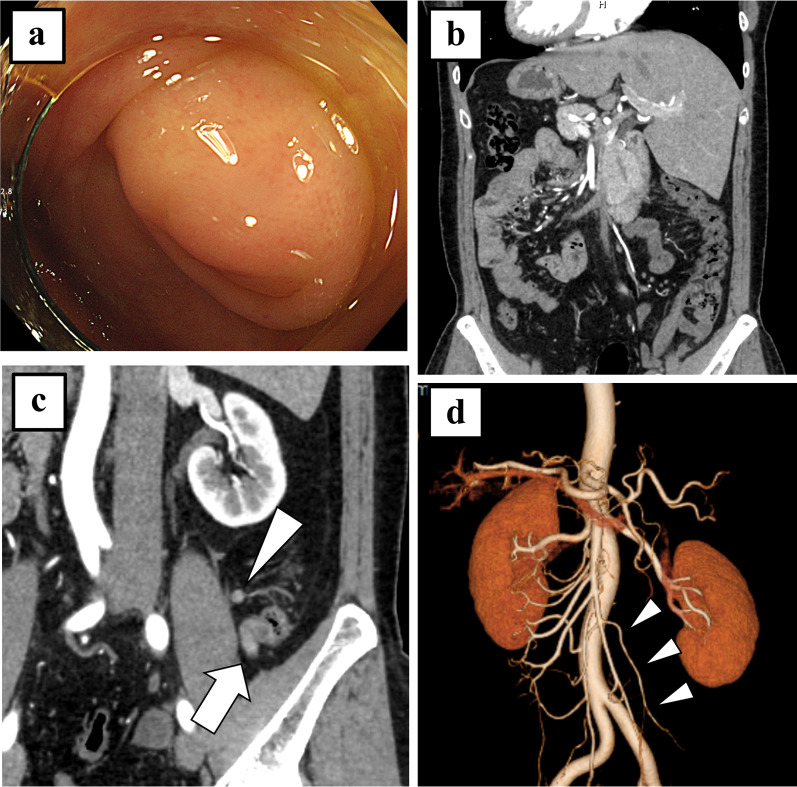
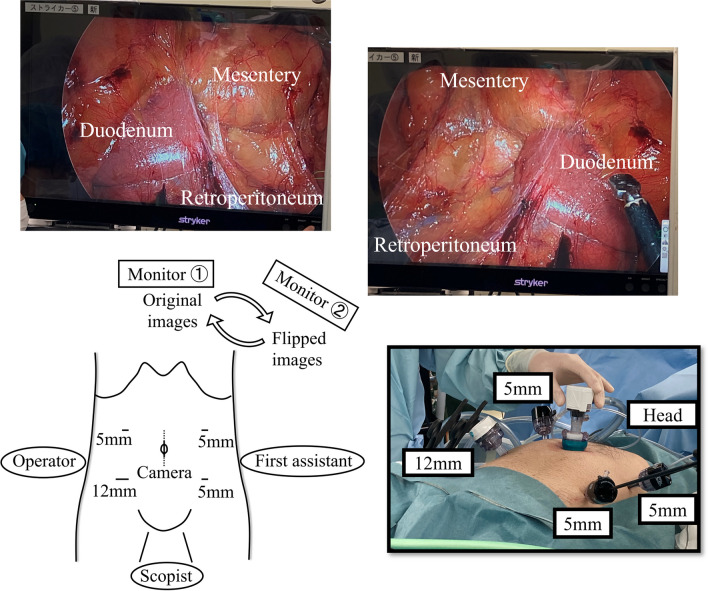
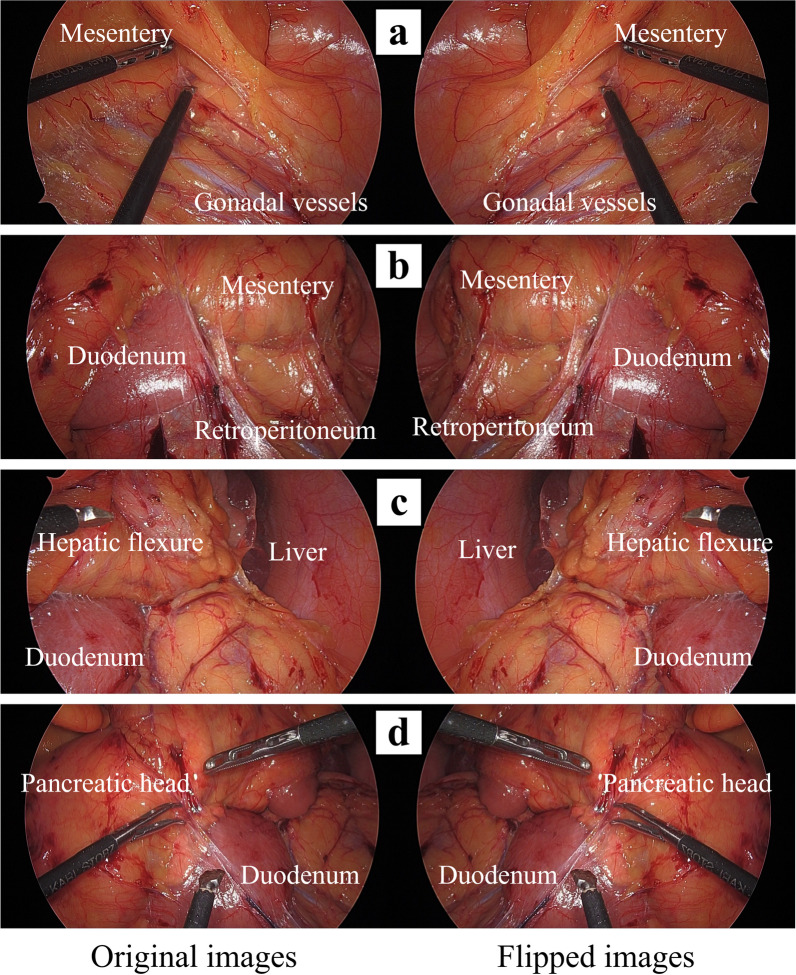
Case presentation: A 41-year-old man with SIT was diagnosed with an appendiceal tumor and underwent laparoscopic-assisted ileocecal resection. Preoperatively, we evaluated anatomical variations using 3D-computed tomography and simulated mirror images by watching flipped videos of patients with normal anatomy undergoing similar operations. During the operation, port placement and the surgeons' standing positions were reversed. Additionally, two monitors were placed at the patient's head, with one monitor showing original images, and the other showing flipped images that looked the same as the normal anatomy. We checked the range of the mobilized region and important anatomical structures by watching the flipped monitor as needed. The patient's postoperative course was uneventful.
Conclusions: Due to the complexities of laparoscopic surgery for SIT, preoperative preparation and surgical innovation are necessary for safe surgery. Several suggestions have been made to understand anatomical anomalies and improve operability; however, surgeons must focus on the mirror-image anatomy throughout the operation. Therefore, the use of intraoperative flipped monitor will be helpful for surgeons in reducing the risk of anatomical misidentification.
Keywords: Intraoperative flipped monitor; Laparoscopic surgery; Situs inversus totalis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Mayo CW, Rice RG. Situs inversus totalis; a statistical review of data on 76 cases with special reference to disease of the biliary tract. Arch Surg. 1920;1949(58):724–730. - PubMed
LinkOut - more resources
Full Text Sources
