

Oral health-related quality of life and survival analysis after preventive and restorative treatment of molar-incisor hypomineralisation
- PMID: 38191504
- PMCID: PMC10774292
- DOI: 10.1038/s41598-024-51223-3
Oral health-related quality of life and survival analysis after preventive and restorative treatment of molar-incisor hypomineralisation
Abstract
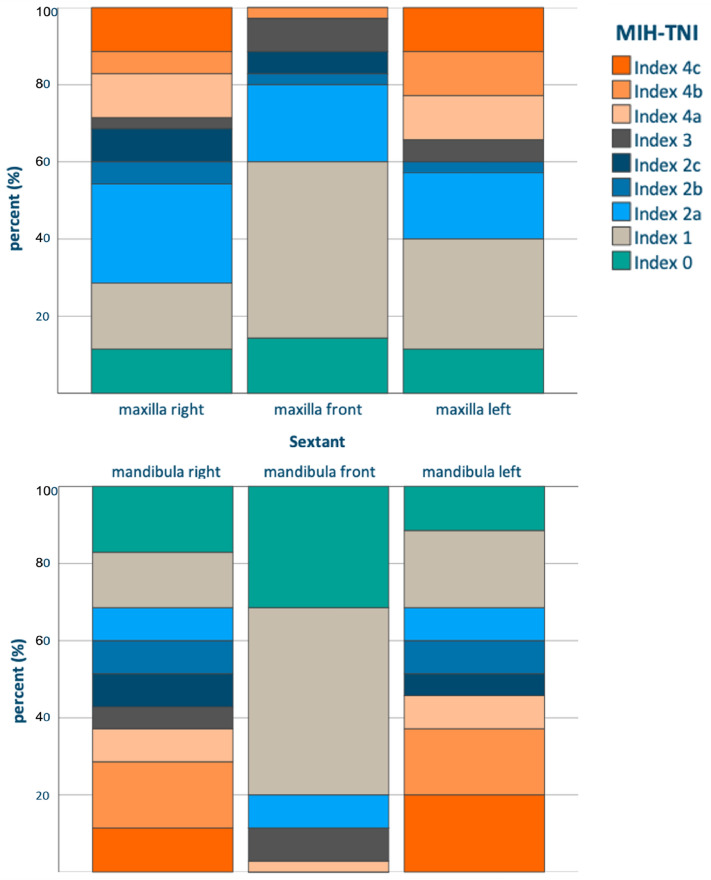
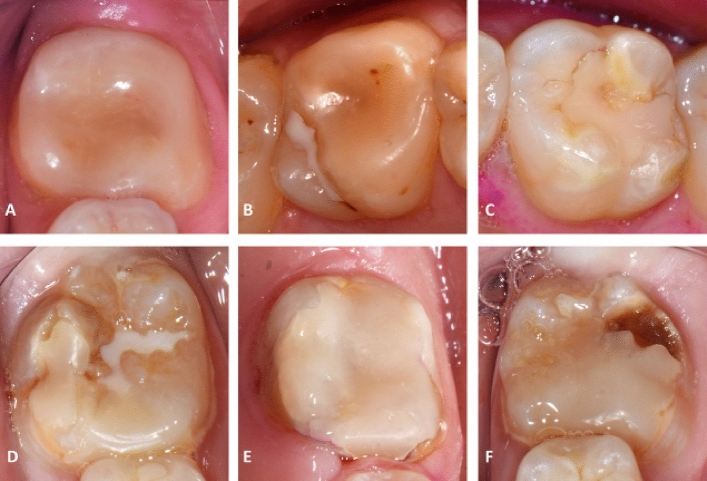
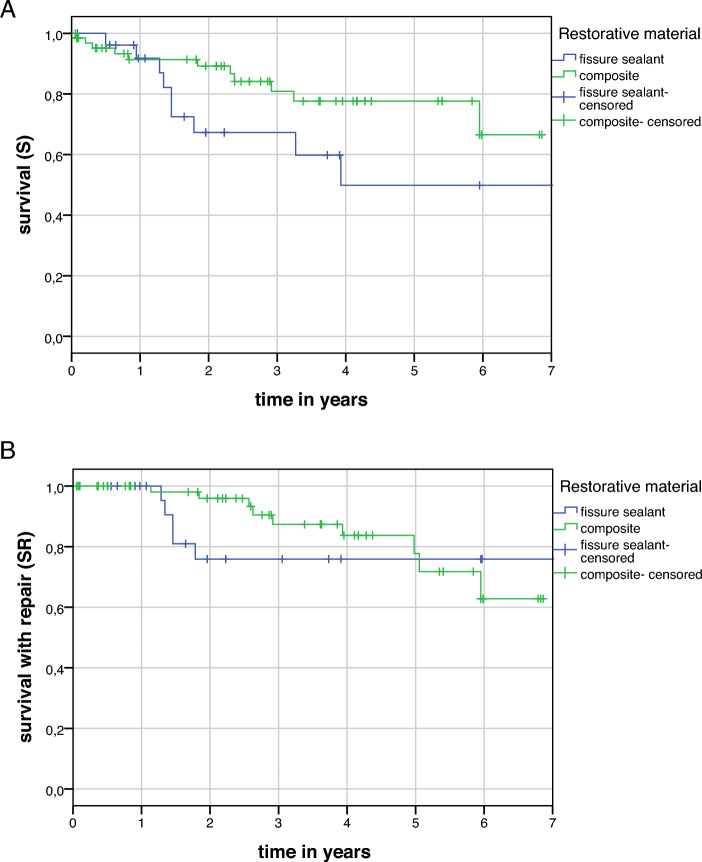
The aim of this study was to assess the impact of molar-incisor hypomineralisation (MIH) on oral health-related quality of life (OHRQoL) in children and adolescents, including information on restorative care, tooth sensitivity, as well as sociodemographic factors. Thirty-five patients aged between 7 and 17 years underwent a comprehensive oral examination. Severity of MIH was graded using the MIH Treatment Need Index (MIH-TNI), OHRQoL using the Child Oral Health Impact Profile (COHIP-19). Clinical quality of restorations was assessed according to modified FDI-criteria, tooth sensitivity using the Schiff Cold Air Sensitivity Scale (SCASS). The mean age was 11.3 ± 3.0 years, 34% were female. On average, 6.9 ± 2.8 teeth were affected, 62,9% had hypersensitive teeth (SCASS ≥ 1). Eighty-nine percent of patients had received restorative care, with a mean of 3.3 ± 2.1 teeth restored, most often with composite, followed by fissure sealing. Nine percent of restorations failed by the FDI-criteria. Mean estimated survival times for success were 4.9 years (95% CI 3.5; 6.2) and 5.6 years (95% CI 5.0; 6.3) for fissure sealants and composite restorations, respectively. The mean COHIP-19 score was 64.3 ± 8.2 (max. possible score = 76). A higher severity of MIH-TNI correlated significantly with impaired OHRQoL (rs = - 0.38, p = 0.013). However, this was not mirrored in multiple regression analysis. Despite the high rate of restorative treatment with an acceptable failure rate, OHRQoL is reduced in children with MIH. Many teeth affected by MIH remain sensitive. Further studies are needed to assess the benefits of different restorative options.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Molar incisor hypomineralization and oral health-related quality of life: a sample of 8-12-years-old children.Clin Oral Investig. 2024 Jan 20;28(1):105. doi: 10.1007/s00784-024-05490-z. Clin Oral Investig. 2024. PMID: 38244077 Free PMC article.
-
Hypersensitivity in teeth affected by molar-incisor hypomineralization (MIH).Sci Rep. 2021 Sep 9;11(1):17922. doi: 10.1038/s41598-021-95875-x. Sci Rep. 2021. PMID: 34504122 Free PMC article.
-
The association between molar incisor hypomineralization and oral health-related quality of life: a cross-sectional study.Clin Oral Investig. 2022 May;26(5):4071-4077. doi: 10.1007/s00784-022-04375-3. Epub 2022 Feb 11. Clin Oral Investig. 2022. PMID: 35147789 Free PMC article.
-
Best clinical practice guidance for clinicians dealing with children presenting with molar-incisor-hypomineralisation (MIH): an updated European Academy of Paediatric Dentistry policy document.Eur Arch Paediatr Dent. 2022 Feb;23(1):3-21. doi: 10.1007/s40368-021-00668-5. Epub 2021 Oct 20. Eur Arch Paediatr Dent. 2022. PMID: 34669177 Free PMC article. Review.
-
Impact of Molar Incisor Hypomineralisation on Quality of Life.Monogr Oral Sci. 2024;32:79-87. doi: 10.1159/000538873. Epub 2024 Jul 1. Monogr Oral Sci. 2024. PMID: 39321780 Review.
Cited by
-
Comparative analysis of oral microbiome in molar-incisor-hypomineralization vs healthy age-matched controls.Microbiol Spectr. 2025 Mar 31;13(5):e0289724. doi: 10.1128/spectrum.02897-24. Online ahead of print. Microbiol Spectr. 2025. PMID: 40162761 Free PMC article.
-
Oral health-related quality of life in Egyptian children with Molar Incisor Hypomineralisation. An observational study.BDJ Open. 2024 Nov 30;10(1):89. doi: 10.1038/s41405-024-00272-x. BDJ Open. 2024. PMID: 39616152 Free PMC article.
-
Efficiency of glass ionomer sealant application in reducing hypersensitivity in MIH-molars in schoolchildren immediately and after 12 weeks.Eur Arch Paediatr Dent. 2025 Apr;26(2):361-373. doi: 10.1007/s40368-024-00988-2. Epub 2025 Jan 17. Eur Arch Paediatr Dent. 2025. PMID: 39821495 Free PMC article.
-
Hypersensitivity associated with molar-incisor hypomineralisation (MIH) among elementary schoolchildren in Bavaria, Germany: results from a cross-sectional study.Eur Arch Paediatr Dent. 2025 Jun 4. doi: 10.1007/s40368-025-01054-1. Online ahead of print. Eur Arch Paediatr Dent. 2025. PMID: 40465132
-
Evaluation of the effect of dental caries, oral hygiene, and treatment need on oral health-related quality of life among Turkish orphan children and adolescents.BMC Oral Health. 2025 Jan 24;25(1):134. doi: 10.1186/s12903-025-05492-7. BMC Oral Health. 2025. PMID: 39856678 Free PMC article.
References
-
- Mast P, Rodrigueztapia MT, Daeniker L, Krejci I. Understanding MIH: Definition, epidemiology, differential diagnosis and new treatment guidelines. Eur. J. Paediatr. Dent. 2013;14:204–208. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
