

Implantable cardioverter defibrillator use in arrhythmogenic right ventricular cardiomyopathy in North America and Europe
- PMID: 38195003
- PMCID: PMC11024811
- DOI: 10.1093/eurheartj/ehad799
Implantable cardioverter defibrillator use in arrhythmogenic right ventricular cardiomyopathy in North America and Europe
Abstract
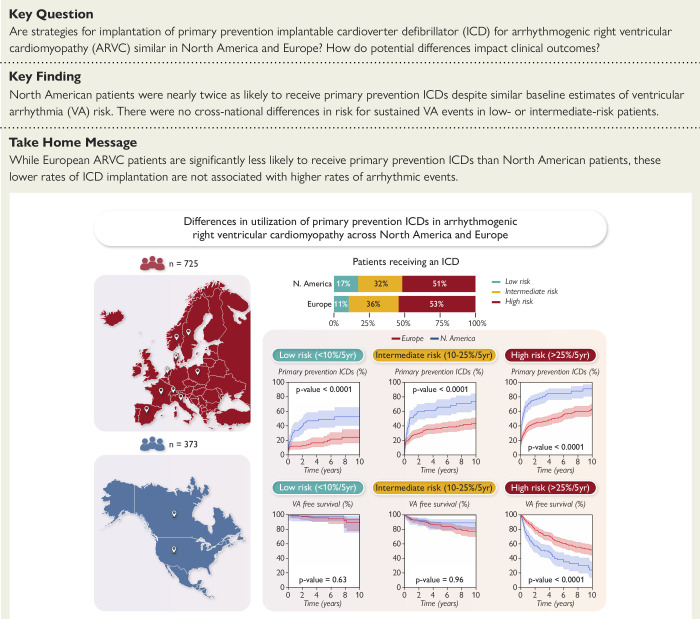
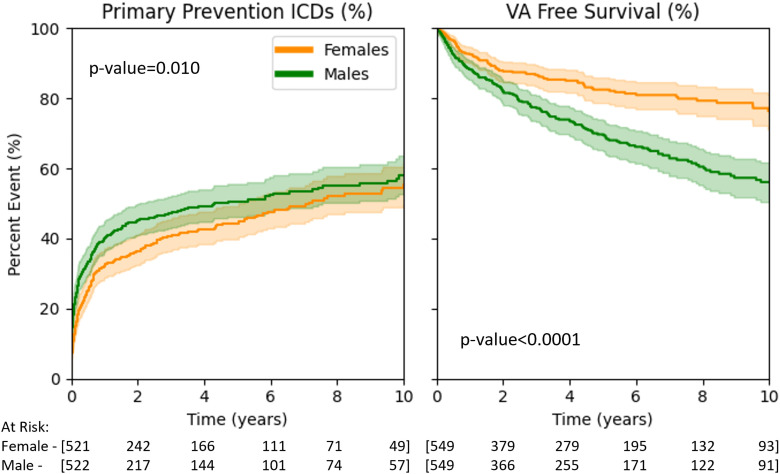
Background and aims: Implantable cardioverter-defibrillators (ICDs) are critical for preventing sudden cardiac death (SCD) in arrhythmogenic right ventricular cardiomyopathy (ARVC). This study aims to identify cross-continental differences in utilization of primary prevention ICDs and survival free from sustained ventricular arrhythmia (VA) in ARVC.
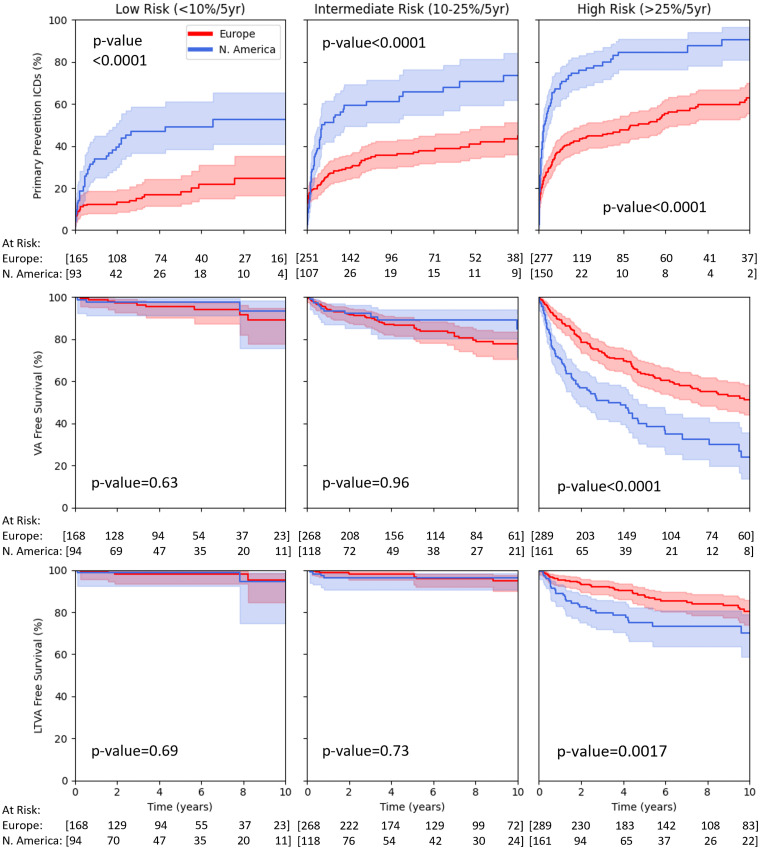
Methods: This was a retrospective analysis of ARVC patients without prior VA enrolled in clinical registries from 11 countries throughout Europe and North America. Patients were classified according to whether they received treatment in North America or Europe and were further stratified by baseline predicted VA risk into low- (<10%/5 years), intermediate- (10%-25%/5 years), and high-risk (>25%/5 years) groups. Differences in ICD implantation and survival free from sustained VA events (including appropriate ICD therapy) were assessed.
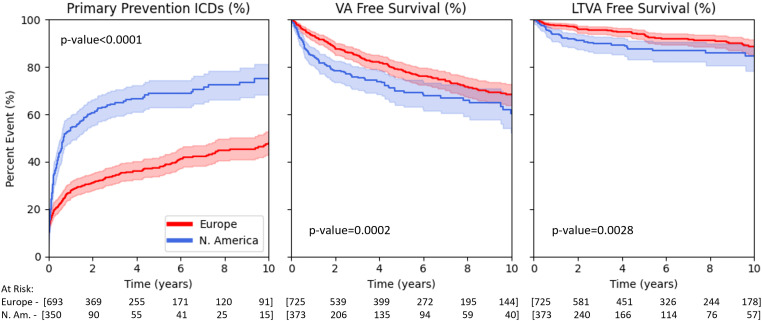
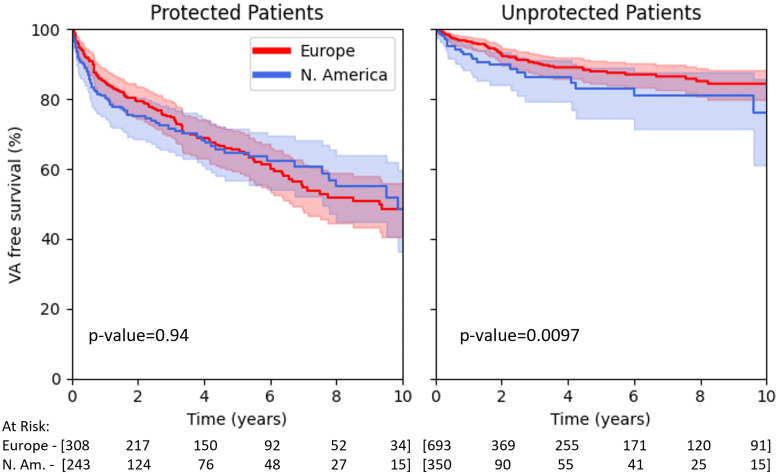
Results: One thousand ninety-eight patients were followed for a median of 5.1 years; 554 (50.5%) received a primary prevention ICD, and 286 (26.0%) experienced a first VA event. After adjusting for baseline risk factors, North Americans were more than three times as likely to receive ICDs {hazard ratio (HR) 3.1 [95% confidence interval (CI) 2.5, 3.8]} but had only mildly increased risk for incident sustained VA [HR 1.4 (95% CI 1.1, 1.8)]. North Americans without ICDs were at higher risk for incident sustained VA [HR 2.1 (95% CI 1.3, 3.4)] than Europeans.
Conclusions: North American ARVC patients were substantially more likely than Europeans to receive primary prevention ICDs across all arrhythmic risk strata. A lower rate of ICD implantation in Europe was not associated with a higher rate of VA events in those without ICDs.
Keywords: Arrhythmogenic right ventricular cardiomyopathy; Implantable cardioverter-defibrillator; Primary prevention; Sudden cardiac death; Ventricular arrhythmia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Olde Nordkamp LR, Postema PG, Knops RE, van Dijk N, Limpens J, Wilde AA, et al. . Implantable cardioverter-defibrillator harm in young patients with inherited arrhythmia syndromes: a systematic review and meta-analysis of inappropriate shocks and complications. Heart Rhythm 2016;13:443–54. 10.1016/j.hrthm.2015.09.010 - DOI - PubMed
-
- Corrado D, Calkins H, Link MS, Leoni L, Favale S, Bevilacqua M, et al. . Prophylactic implantable defibrillator in patients with arrhythmogenic right ventricular cardiomyopathy/dysplasia and no prior ventricular fibrillation or sustained ventricular tachycardia. Circulation 2010;122:1144–52. 10.1161/CIRCULATIONAHA.109.913871 - DOI - PubMed
-
- Bhonsale A, James CA, Tichnell C, Murray B, Gagarin D, Philips B, et al. . Incidence and predictors of implantable cardioverter-defibrillator therapy in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy undergoing implantable cardioverter-defibrillator implantation for primary prevention. J Am Coll Cardiol 2011;58:1485–96. 10.1016/j.jacc.2011.06.043 - DOI - PubMed
