

Health effects associated with exposure to secondhand smoke: a Burden of Proof study
- PMID: 38195750
- PMCID: PMC10803272
- DOI: 10.1038/s41591-023-02743-4
Health effects associated with exposure to secondhand smoke: a Burden of Proof study
Erratum in
-
Author Correction: Health effects associated with exposure to secondhand smoke: a Burden of Proof study.Nat Med. 2024 Apr;30(4):1213. doi: 10.1038/s41591-024-02832-y. Nat Med. 2024. PMID: 38291302 Free PMC article. No abstract available.
Abstract
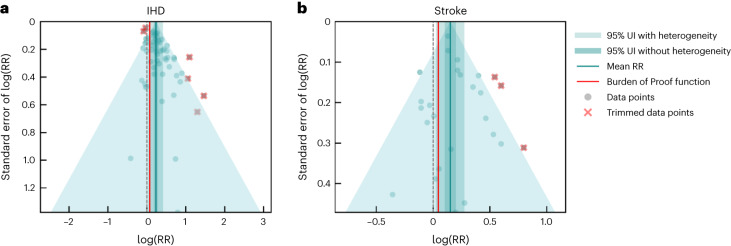
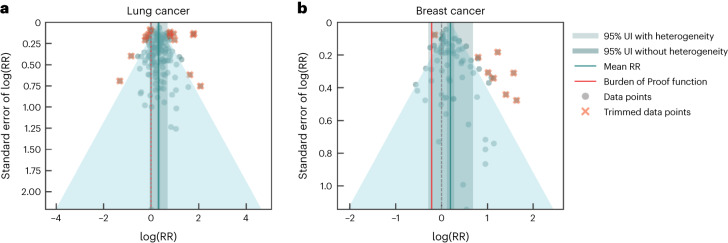
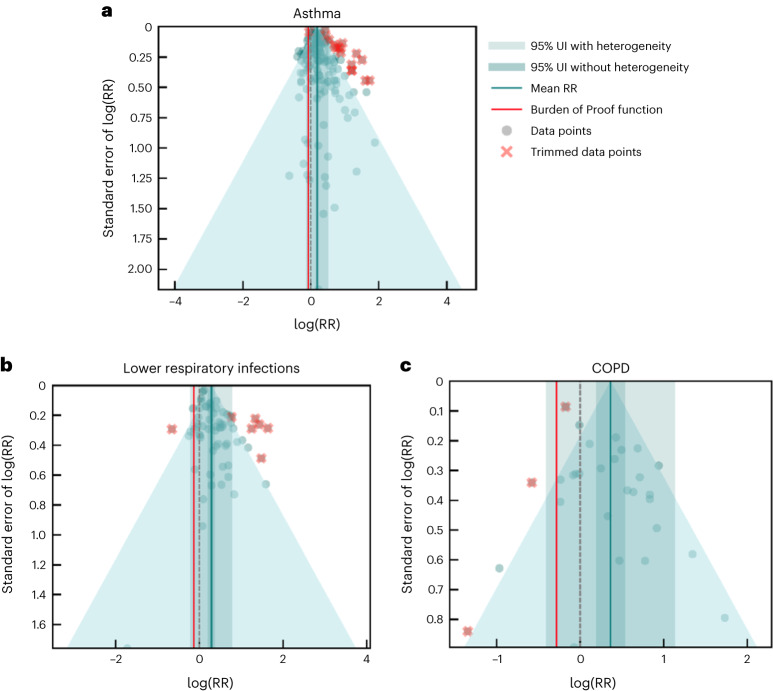
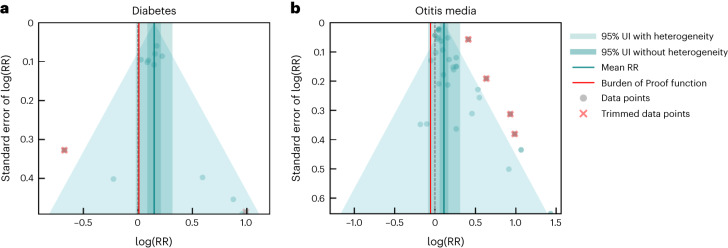
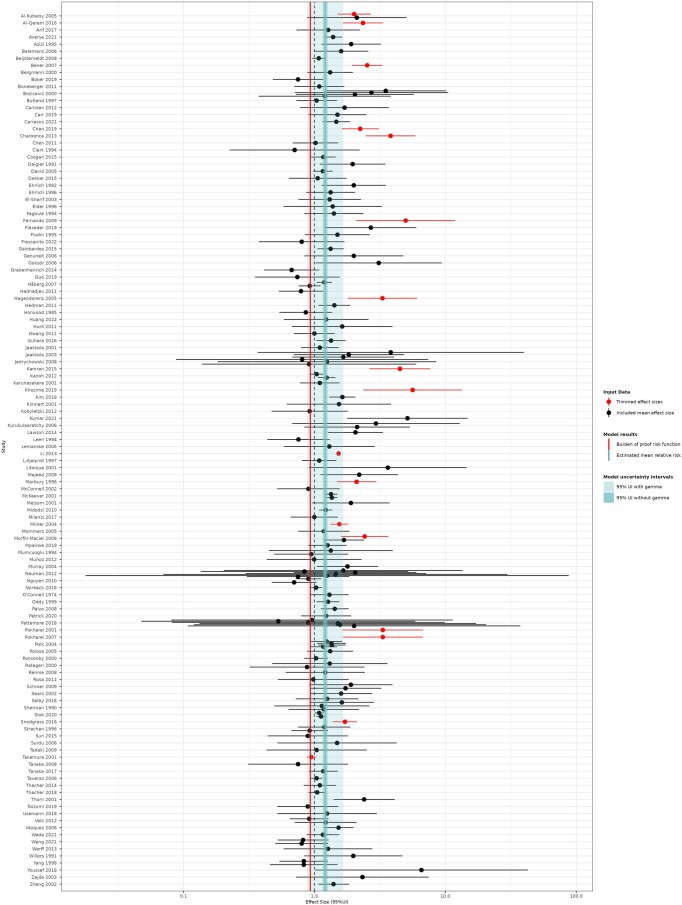
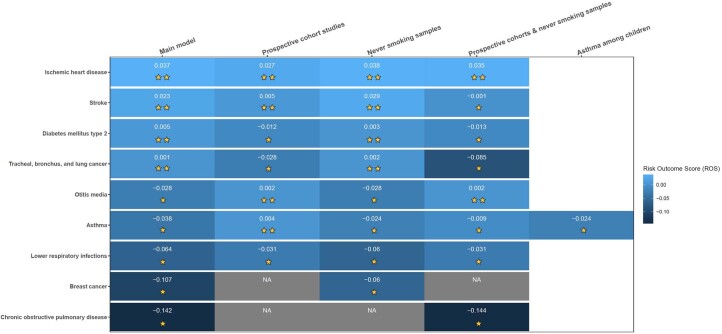
Despite a gradual decline in smoking rates over time, exposure to secondhand smoke (SHS) continues to cause harm to nonsmokers, who are disproportionately children and women living in low- and middle-income countries. We comprehensively reviewed the literature published by July 2022 concerning the adverse impacts of SHS exposure on nine health outcomes. Following, we quantified each exposure-response association accounting for various sources of uncertainty and evaluated the strength of the evidence supporting our analyses using the Burden of Proof Risk Function methodology. We found all nine health outcomes to be associated with SHS exposure. We conservatively estimated that SHS increases the risk of ischemic heart disease, stroke, type 2 diabetes and lung cancer by at least around 8%, 5%, 1% and 1%, respectively, with the evidence supporting these harmful associations rated as weak (two stars). The evidence supporting the harmful associations between SHS and otitis media, asthma, lower respiratory infections, breast cancer and chronic obstructive pulmonary disease was weaker (one star). Despite the weak underlying evidence for these associations, our results reinforce the harmful effects of SHS on health and the need to prioritize advancing efforts to reduce active and passive smoking through a combination of public health policies and education initiatives.
© 2024. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no competing interests.
Figures








References
-
- Gakidou E, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1345–1422. doi: 10.1016/S0140-6736(17)32366-8. - DOI - PMC - PubMed
-
- How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General (US Department of Health and Human Services, 2010). - PubMed
