

Lung cancer in patients who have never smoked - an emerging disease
- PMID: 38195910
- PMCID: PMC11014425
- DOI: 10.1038/s41571-023-00844-0
Lung cancer in patients who have never smoked - an emerging disease
Abstract
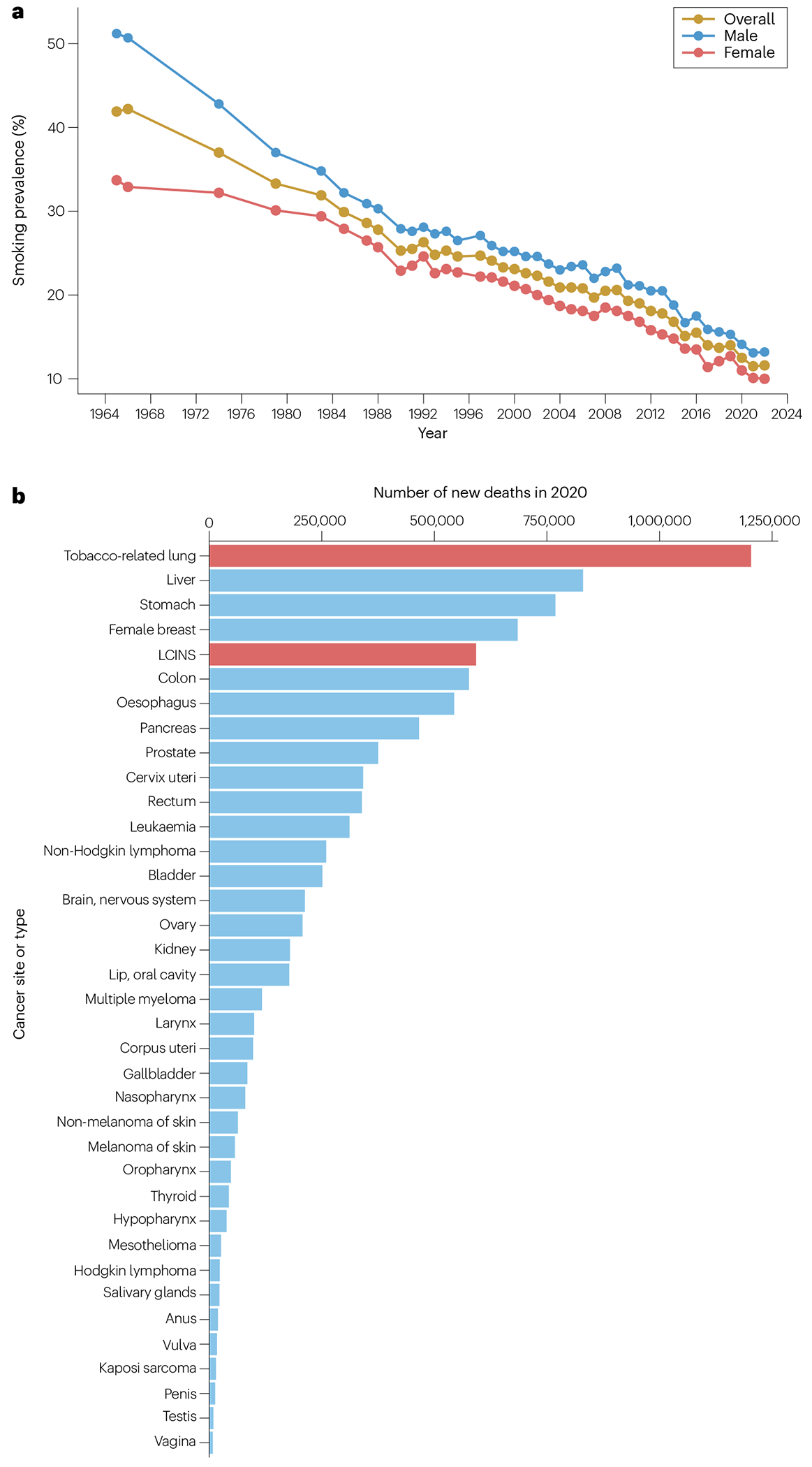
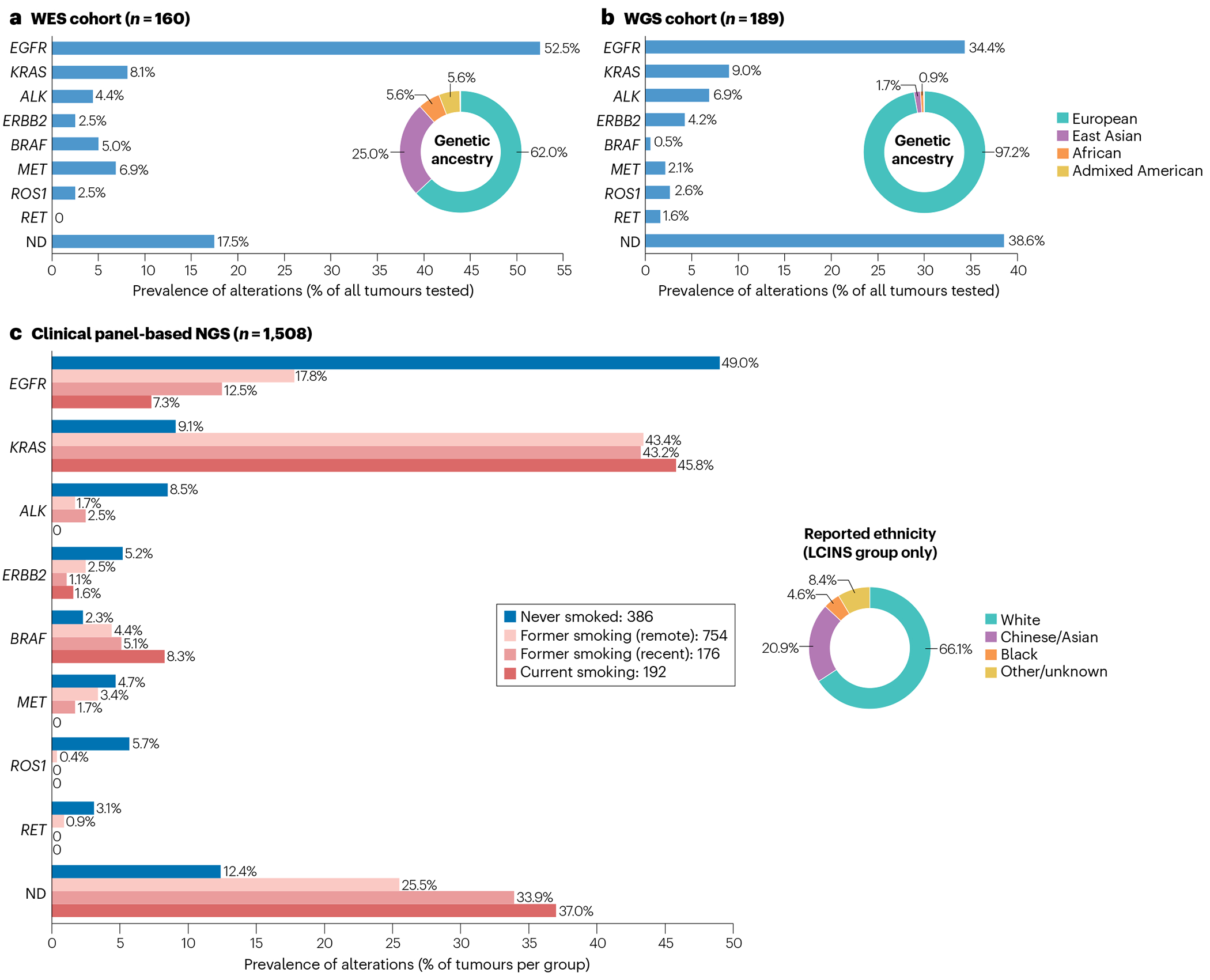
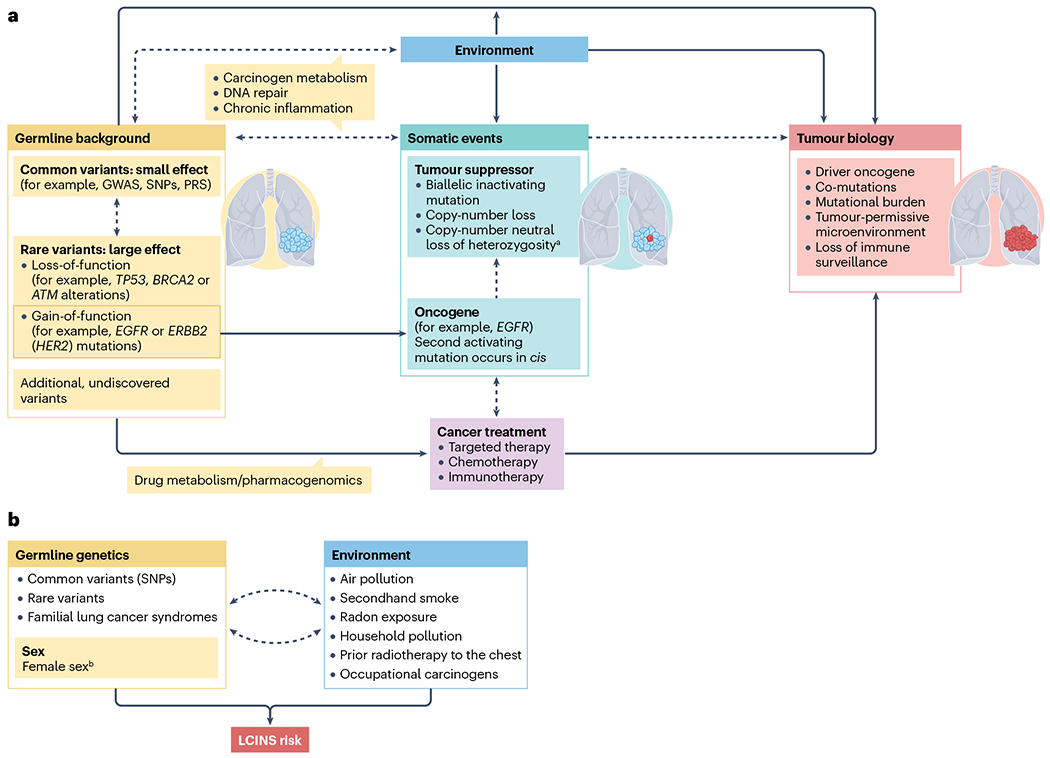
Lung cancer is the most common cause of cancer-related deaths globally. Although smoking-related lung cancers continue to account for the majority of diagnoses, smoking rates have been decreasing for several decades. Lung cancer in individuals who have never smoked (LCINS) is estimated to be the fifth most common cause of cancer-related deaths worldwide in 2023, preferentially occurring in women and Asian populations. As smoking rates continue to decline, understanding the aetiology and features of this disease, which necessitate unique diagnostic and treatment paradigms, will be imperative. New data have provided important insights into the molecular and genomic characteristics of LCINS, which are distinct from those of smoking-associated lung cancers and directly affect treatment decisions and outcomes. Herein, we review the emerging data regarding the aetiology and features of LCINS, particularly the genetic and environmental underpinnings of this disease as well as their implications for treatment. In addition, we outline the unique diagnostic and therapeutic paradigms of LCINS and discuss future directions in identifying individuals at high risk of this disease for potential screening efforts.
© 2024. Springer Nature Limited.
Conflict of interest statement
Competing interests
P.A.J. declares consultancy roles for Abbvie, Accutar Biotech, Allorion Therapeutics, AstraZeneca, Bayer, Biocartis, Boehringer Ingelheim, Chugai Pharmaceuticals, Daiichi Sankyo, DualityBio, Eisai, Eli Lilly, Frontier Medicines, Hongyun Biotechnology, Merus, Mirati Therapeutics, Monte Rosa, Novartis, Nuvalent, Pfizer, Roche/Genentech, Sanofi, Scorpion Therapeutics, SFJ Pharmaceuticals, Silicon Therapeutics, Syndax, Takeda Oncology, Transcenta and Voronoi; stock ownership in Gatekeeper Pharmaceuticals; research funding from AstraZenenca, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, PUMA Biotechnology, Revolution Medicines and Takeda Oncology; and post-marketing royalties from Dana-Farber Cancer Institute-owned intellectual property relating to
Figures
References
-
- Siegel RL, Miller KD, Wagle NS & Jemal A Cancer statistics, 2023. CA Cancer J. Clin 73, 17–48 (2023). - PubMed
-
- The American Lung Association. Overall Tobacco Trends. Analysis of Centers for Disease Control and Prevention, National Center for Health Statistics. National Health Interview Survey 1965-2018. lung.org, https://www.lung.org/research/trends-in-lung-disease/tobacco-trends-brie... (2019).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
