

This is a preprint.
Risk of Atherosclerotic Cardiovascular Disease Hospitalizations after COPD Hospitalization among Older Adults
- PMID: 38196600
- PMCID: PMC10775335
- DOI: 10.1101/2023.12.19.23300254
Risk of Atherosclerotic Cardiovascular Disease Hospitalizations after COPD Hospitalization among Older Adults
Update in
-
Risk of Atherosclerotic Cardiovascular Disease Hospitalizations after Chronic Obstructive Pulmonary Disease Hospitalization among Older Adults.Ann Am Thorac Soc. 2024 Nov;21(11):1516-1523. doi: 10.1513/AnnalsATS.202401-017OC. Ann Am Thorac Soc. 2024. PMID: 39018486
Abstract
Background: Meta-analyses have suggested the risk of atherosclerotic cardiovascular disease (ASCVD) events is significantly higher after a chronic obstructive pulmonary disease (COPD) exacerbation. However, these studies have been limited to highly selected patient populations potentially not generalizable to the broader population of COPD.
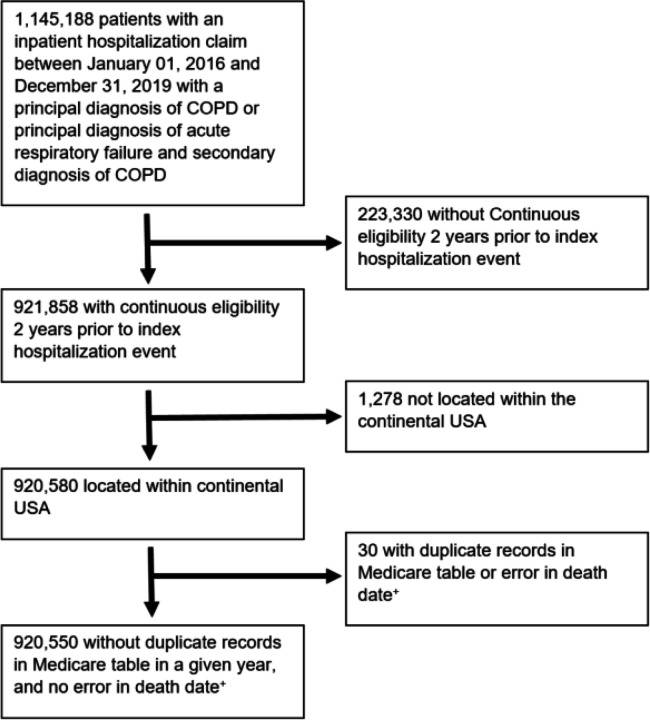
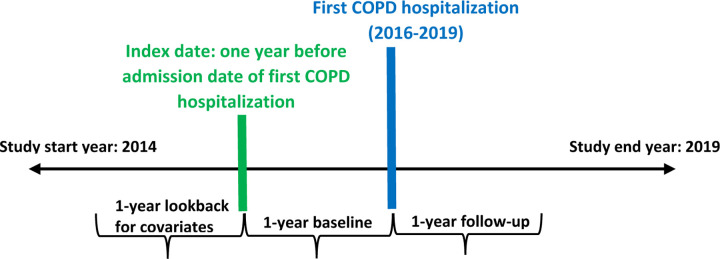
Methods: We assessed the risk of ASCVD hospitalizations after COPD hospitalization compared to before COPD hospitalization and identified patient factors associated with ASCVD hospitalizations after COPD hospitalization. This retrospective cohort study used claims data from 920,550 Medicare beneficiaries hospitalized for COPD from 2016-2019 in the US. The primary outcome was risk of a ASCVD hospitalization composite outcome (myocardial infarction, percutaneous coronary intervention, coronary artery by-pass graft surgery, stroke, or transient ischemic attack) in the 1 year after-COPD hospitalization relative to the 1 year before-COPD hospitalization. Time from discharge to a composite ASCVD hospitalization outcome was modeled using an extension of the Cox Proportional-Hazards model, the Anderson-Gill model with adjustment for patient characteristics. Additional analyses evaluated for interactions in subgroups and risk factors associated with the composite ASCVD hospitalization outcome.
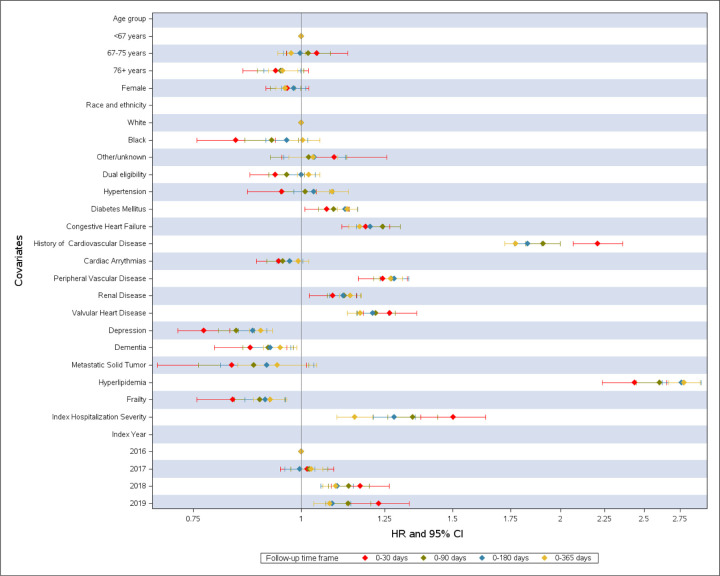
Results: Among 920,550 patients (mean age, 73 years) the hazard ratio estimate (HR; 95% CI) for the composite ASCVD hospitalization outcome after-COPD hospitalization vs before-COPD hospitalization was 0.99 (0.97, 1.02; p = 0.53) following adjustment. We observed 3 subgroups that were significantly associated with higher risk for ASCVD hospitalizations after COPD hospitalization: 76+ years old, women, COPD hospitalization severity. Among the 19 characteristics evaluated, 10 were significantly associated with higher risk of CVD events 1 year after COPD hospitalization with hyperlipidemia (2.78; 2.67, 2.90) and history of cardiovascular disease (1.77; 1.72 1.83) associated with the greatest risk.
Conclusion: Among Medicare beneficiaries hospitalized for COPD, the risk of ASCVD hospitalizations was not significantly increased after COPD-hospitalization relative to before-COPD hospitalization. Although, we identified age 76+ years old, female sex, and COPD hospitalization severity as high risk subgroups and 10 risk factors associated with increased risk of ASCVD events after-COPD hospitalization. Further research is needed to characterize the COPD exacerbation populations at highest ASCVD hospitalization risk.
Figures

References
-
- Çolak Y, Afzal S, Marott JL, Nordestgaard BG, Vestbo J, Ingebrigtsen TS and Lange P. Prognosis of COPD depends on severity of exacerbation history: A population-based analysis. Respiratory medicine. 2019;155:141–147. - PubMed
-
- Reilev M, Pottegård A, Lykkegaard J, Søndergaard J, Ingebrigtsen TS and Hallas J. Increased risk of major adverse cardiac events following the onset of acute exacerbations of COPD. Respirology (Carlton, Vic). 2019;24:1183–1190. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources