

Development and Implementation of an Escalation Protocol for Internal Medicine Trainees
- PMID: 38196684
- PMCID: PMC10773492
- DOI: 10.34197/ats-scholar.2023-0009IN
Development and Implementation of an Escalation Protocol for Internal Medicine Trainees
Abstract
Background: Overnight, physicians in training receive less direct supervision. Decreased direct supervision requires trainees to appropriately assess patients at risk of clinical deterioration and escalate to supervising physicians. Failure of trainees to escalate contributes to adverse patient safety events.
Objective: To standardize the evaluation of patients at risk of deterioration overnight by internal medicine residents, increase communication between residents and supervising physicians, and improve perceptions of patient safety at a tertiary academic medical center.
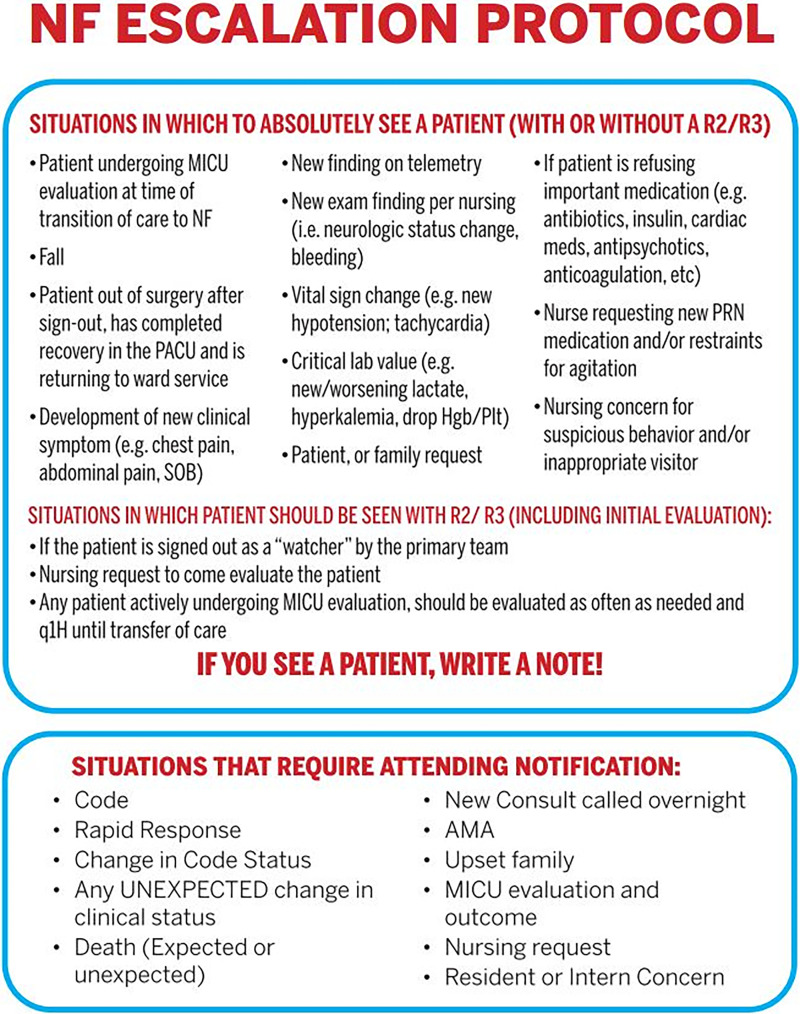
Methods: A multidisciplinary stakeholder team developed an overnight escalation-of-care protocol for residents. The protocol was implemented with badge buddies and an educational campaign targeted at residents, supervising physicians, and nursing staff. Residents and supervising physicians completed anonymous surveys to assess the use of the protocol; the frequency of overnight communication between residents and supervising physicians; and perceptions of escalation and patient safety before, immediately after ("early postintervention"), and 8 months after ("delayed postintervention") the intervention.
Results: Seventy-five (100%) residents participated in the intervention, and 57-89% of those invited to complete surveys at the various time points responded. After the intervention, 82% of residents reported using the protocol, though no change was observed in the frequency of communication between residents and supervising physicians. After the implementation, residents perceived that patient care was safer (early postintervention, 47%; delayed postintervention, 72%; P = 0.02), and interns expressed decreased fear of waking and being criticized by supervising physicians.
Conclusion: An escalation-of-care protocol was developed and successfully implemented using a multimodal approach. The implementation and dissemination of the protocol standardized resident escalation overnight and improved resident-perceived patient safety and interns' comfort with escalation.
Keywords: clinical deterioration; communication; escalation of care; patient safety; residency training.
Copyright © 2023 by the American Thoracic Society.
Figures

References
-
- Halpern SD, Detsky AS. Graded autonomy in medical education—managing things that go bump in the night. N Engl J Med . 2014;370:1086–1089. - PubMed
-
- Burke JR, Downey C, Almoudaris AM. Failure to rescue deteriorating patients: a systematic review of root causes and improvement strategies. J Patient Saf . 2022;18:e140–e155. - PubMed
-
- Johnston MJ, Arora S, King D, Bouras G, Almoudaris AM, Davis R, et al. A systematic review to identify the factors that affect failure to rescue and escalation of care in surgery. Surgery . 2015;157:752–763. - PubMed
-
- Farnan JM, Johnson JK, Meltzer DO, Humphrey HJ, Arora VM. On-call supervision and resident autonomy: from micromanager to absentee attending. Am J Med . 2009;122:784–788. - PubMed
-
- Kilminster S, Cottrell D, Grant J, Jolly B. AMEE guide no. 27: effective educational and clinical supervision. Med Teach . 2007;29:2–19. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
