

Patellar Base Support Technique During Manipulation Under Anesthesia for Knee Arthrofibrosis Limits the Risk of Iatrogenic Complications
- PMID: 38196877
- PMCID: PMC10773232
- DOI: 10.1016/j.eats.2023.08.001
Patellar Base Support Technique During Manipulation Under Anesthesia for Knee Arthrofibrosis Limits the Risk of Iatrogenic Complications
Abstract
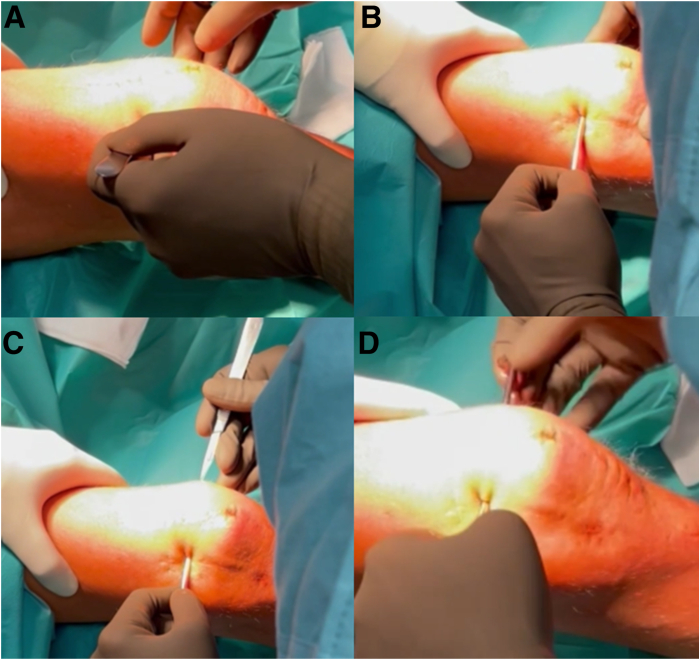
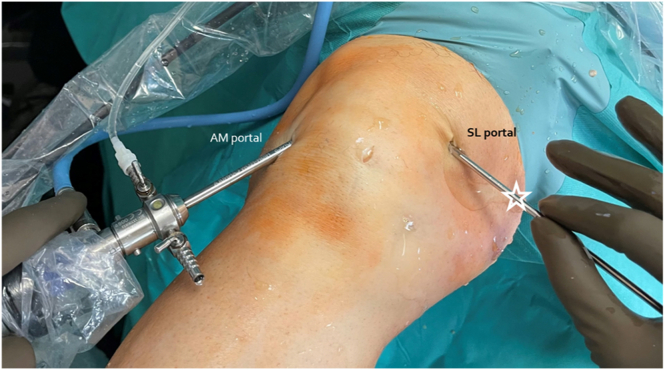
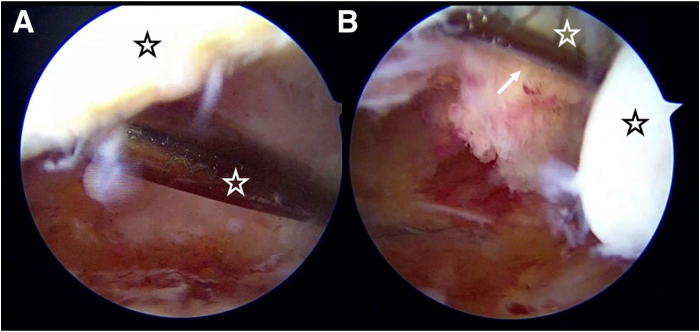
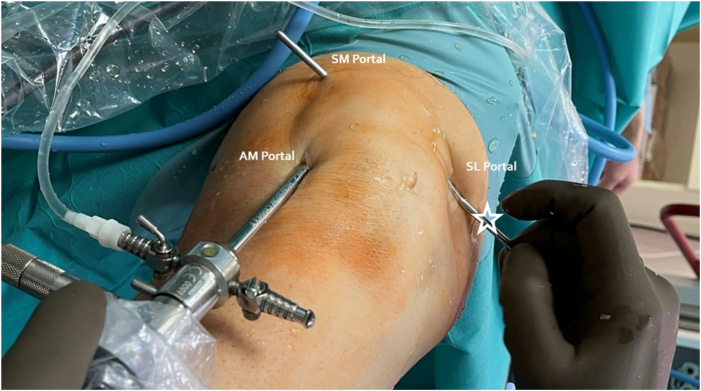
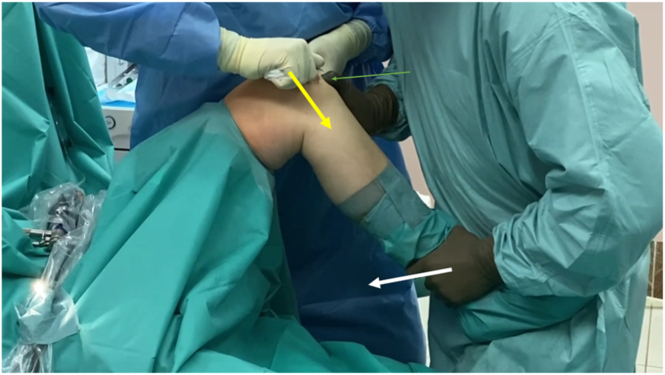
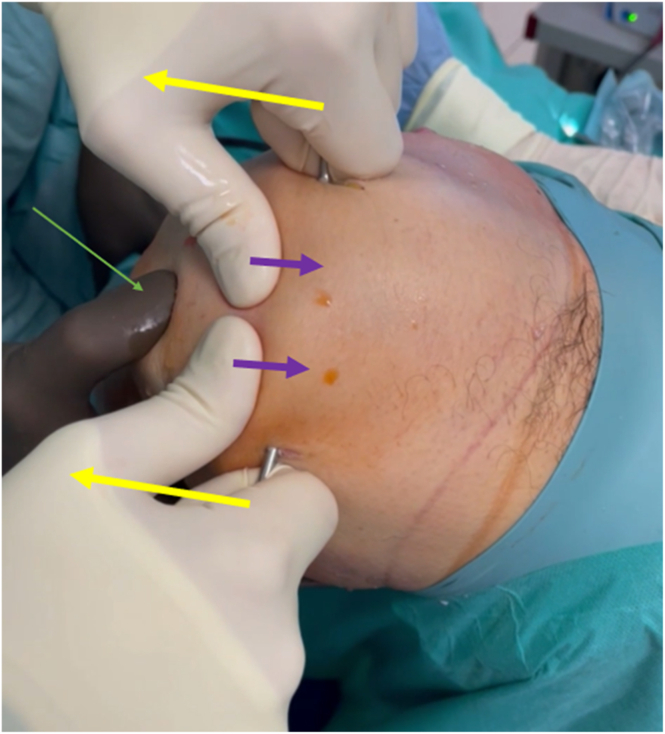
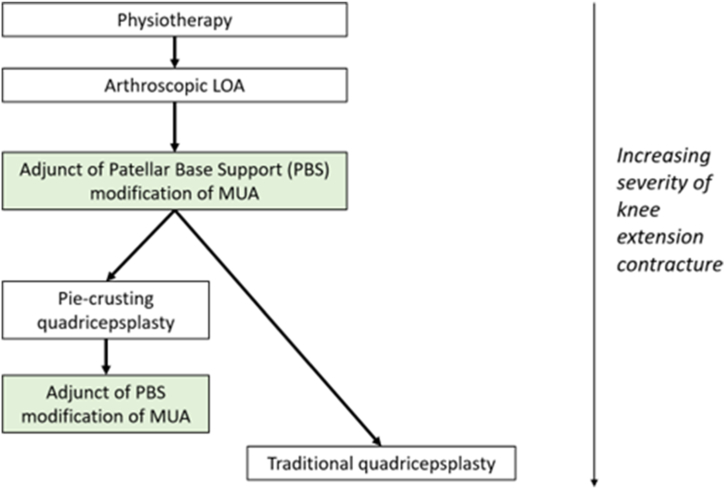
Knee extension contracture is a common postinjury and postsurgical complication, which decreases knee joint flexion. Many techniques have been described in the literature to restore knee flexion, with the most common one being an arthroscopic lysis of adhesions. However, in severe cases, additional intra- and extra-articular procedures are needed to restore full knee flexion. Manipulation under anesthesia (MUA) is one of them. Unfortunately, it may lead to devastating complications, such as iatrogenic rupture of the patellar tendon or fractures of the patella or tibial tuberosity. Therefore, the purpose of this report is to present a safer modification of MUA for knee extension contracture in cases in which excessive force is demanded to achieve flexion. The key aim of the "patellar base support" technique (PBS technique) is to stretch the contracted quadriceps muscle with controlled and decreased tension on the patella, patellar tendon, and tibial tuberosity.
© 2023 The Authors.
Figures
Similar articles
-
Manipulation under anaesthesia versus lysis of adhesions for arthrofibrosis of the knee: a 6-month randomized, multicentre, non-inferiority comparative effectiveness protocol.Ann Palliat Med. 2021 May;10(5):5908-5918. doi: 10.21037/apm-21-48. Epub 2021 Apr 15. Ann Palliat Med. 2021. PMID: 33894738
-
Manipulation Under Anesthesia With Lysis of Adhesions Is Effective in Arthrofibrosis After Sulcus-Deepening Trochleoplasty: A Prospective Study.Orthop J Sports Med. 2019 Aug 23;7(8):2325967119864868. doi: 10.1177/2325967119864868. eCollection 2019 Aug. Orthop J Sports Med. 2019. PMID: 31489329 Free PMC article.
-
Rotating Hinge Revision Total Knee Arthroplasty for Severe Arthrofibrosis.JBJS Essent Surg Tech. 2021 Dec 22;11(4):e21.00009. doi: 10.2106/JBJS.ST.21.00009. eCollection 2021 Oct-Dec. JBJS Essent Surg Tech. 2021. PMID: 35693134 Free PMC article.
-
[Arthrolysis for chronic flexion deficits of the knee. An overview of indications and techniques of vastus intermedius muscle resection, transposition of the tibial tuberosity and z-plasty of the patellar tendon].Unfallchirurg. 2006 Apr;109(4):285-96. doi: 10.1007/s00113-005-1039-4. Unfallchirurg. 2006. PMID: 16391934 Review. German.
-
[Radiologic assessment of femoro-patellar instability. Personal experience and review of the literature].Radiol Med. 2001 Jan-Feb;101(1-2):66-74. Radiol Med. 2001. PMID: 11360756 Review. Italian.
Cited by
-
Patella Baja Revisited: Interposition of a Pedunculated Flap of the Hoffa Fat Pad to Treat Adhesions Between the Tibia and Patellar Tendon and Restore the Functional Length of the Patellar Tendon.Arthrosc Tech. 2024 Jul 2;13(11):103108. doi: 10.1016/j.eats.2024.103108. eCollection 2024 Nov. Arthrosc Tech. 2024. PMID: 39711910 Free PMC article.
References
-
- Pujol N., Boisrenoult P., Beaufils P. Post-traumatic knee stiffness: Surgical techniques. Orthop Traumatol Surg Res. 2015;101:S179–S186. - PubMed
-
- Agarwal A.R., Harris A.B., Tarawneh O., et al. Delay of timing of anterior cruciate ligament reconstruction is associated with lower risk of arthrofibrosis requiring intervention. Arthroscopy. 2023;39:1682–1689.e2. - PubMed
-
- Baghdadi S., Ganley T.J., Wells L., Lawrence J.T.R. Early identification of arthrofibrosis in adolescents following anterior cruciate ligament reconstruction is associated with the need for subsequent surgery: A matched case-control study. Arthroscopy. 2022;38:2278–2286. - PubMed
-
- Young B.L., Hammond K.E. Editorial commentary: Limited preoperative range of motion is associated with range of motion deficits after anterior cruciate ligament reconstruction: “If the knee is not straight, wait.”. Arthroscopy. 2023;39:1690–1691. - PubMed
LinkOut - more resources
Full Text Sources
