

Validation of Echocardiographic Measurements in Patients with Pulmonary Embolism in the RIETE Registry
- PMID: 38197015
- PMCID: PMC10774011
- DOI: 10.1055/s-0043-1777765
Validation of Echocardiographic Measurements in Patients with Pulmonary Embolism in the RIETE Registry
Abstract
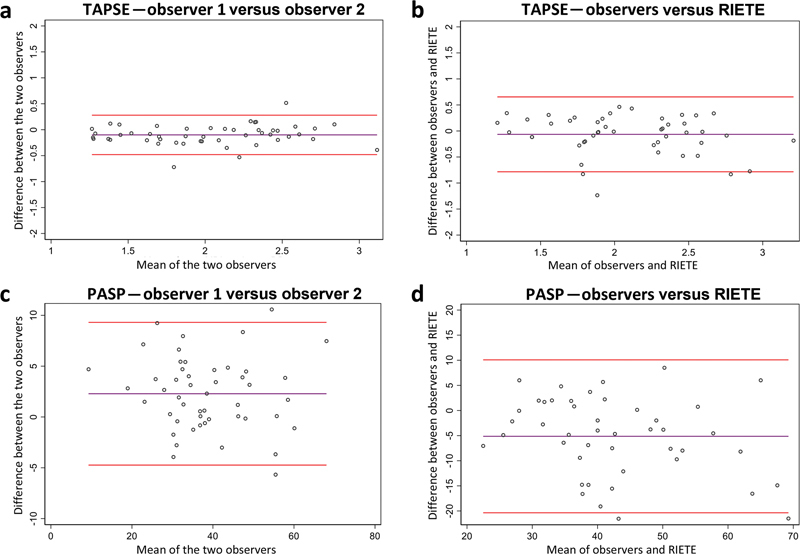
Background In acute pulmonary embolism (PE), echocardiographic identification of right ventricular (RV) dysfunction will inform prognostication and clinical decision-making. Registro Informatizado Enfermedad TromboEmbolica (RIETE) is the world's largest registry of patients with objectively confirmed PE. The reliability of site-reported RV echocardiographic measurements is unknown. We aimed to validate site-reported key RV echocardiographic measurements in the RIETE registry. Methods Fifty-one randomly chosen patients in RIETE who had transthoracic echocardiogram (TTE) performed for acute PE were included. TTEs were de-identified and analyzed by a core laboratory of two independent observers blinded to site-reported data. To investigate reliability, intraclass correlation coefficients (ICCs) and Bland-Altman plots between the two observers, and between an average of the two observers and the RIETE site-reported data were obtained. Results Core laboratory interobserver variations were very limited with correlation coefficients >0.8 for all TTE parameters. Agreement was substantial between core laboratory observers and site-reported data for key parameters including tricuspid annular plane systolic excursion (ICC 0.728; 95% confidence interval [CI], 0.594-0.862) and pulmonary arterial systolic pressure (ICC 0.726; 95% CI, 0.601-0.852). Agreement on right-to-left ventricular diameter ratio (ICC 0.739; 95% CI, 0.443-1.000) was validated, although missing data limited the precision of the estimates. Bland-Altman plots showed differences close to zero. Conclusion We showed substantial reliability of key RV site-reported measurements in the RIETE registry. Ascertaining the validity of such data adds confidence and reliability for subsequent investigations.
Keywords: echocardiography; pulmonary circulation; reliability; right ventricular function; validity.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of Interests B.B. is supported by a Career Development Award from the American Heart Association and VIVA Physicians (#938814) for the PE-EHR+ study. B.B. was also supported by the Scott Schoen and Nancy Adams IGNITE Award, and the Mary Ann Tynan Research Scientist award from the Mary Horrigan Connors Center for Women's Health and Gender Biology at Brigham and Women's Hospital, and the Heart and Vascular Center Junior Faculty Award from Brigham and Women's Hospital. B.B. reports that he is a consulting expert, on behalf of the plaintiff, for litigation related to two specific brand models of IVC filters. C.K. has no conflicts of interest related to this analysis. However, he does report receiving grant funding paid to his institution from Grifols and Diagnostica Stago, as well as consulting fees from BMS/Pfizer. D.J. has no conflicts of interest related to this analysis. However, he does report serving as a speaker for BMS/Pfizer. M.M. received unrestricted grants for research to sponsor the RIETE registry by Sanofi, Bayer, Leo, and Rovi. He also participated in advisory meeting for Sanofi and BMS/Pfizer. E.P.D. has no conflicts of interest related to this analysis.However, she has received speaker fees and participated in advisory meetings led by Pfizer/BMS. The remaining authors have no conflicts of interest to declare.
Figures



References
-
- ESC Scientific Document Group . Konstantinides S V, Meyer G, Becattini C et al.2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur Heart J. 2020;41(04):543–603. - PubMed
-
- Wood K E. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002;121(03):877–905. - PubMed
-
- American Heart Association Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; and Council on Cardiovascular Surgery and Anesthesia . Konstam M A, Kiernan M S, Bernstein D et al.Evaluation and management of right-sided heart failure: a scientific statement from the American Heart Association. Circulation. 2018;137(20):e578–e622. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources