

Repotrectinib in ROS1 Fusion-Positive Non-Small-Cell Lung Cancer
- PMID: 38197815
- PMCID: PMC11702311
- DOI: 10.1056/NEJMoa2302299
Repotrectinib in ROS1 Fusion-Positive Non-Small-Cell Lung Cancer
Abstract
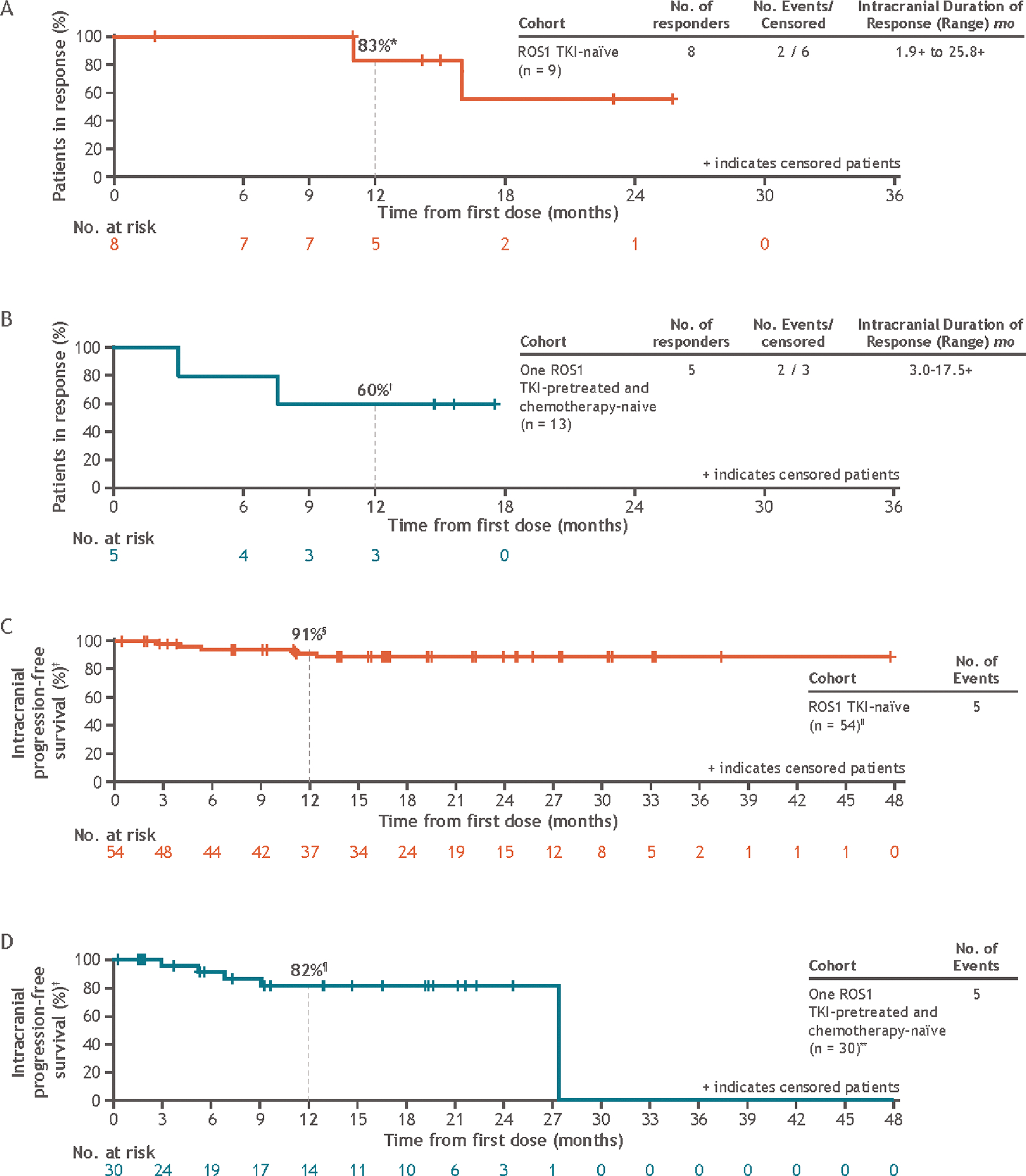
Background: The early-generation ROS1 tyrosine kinase inhibitors (TKIs) that are approved for the treatment of ROS1 fusion-positive non-small-cell lung cancer (NSCLC) have antitumor activity, but resistance develops in tumors, and intracranial activity is suboptimal. Repotrectinib is a next-generation ROS1 TKI with preclinical activity against ROS1 fusion-positive cancers, including those with resistance mutations such as ROS1 G2032R.
Methods: In this registrational phase 1-2 trial, we assessed the efficacy and safety of repotrectinib in patients with advanced solid tumors, including ROS1 fusion-positive NSCLC. The primary efficacy end point in the phase 2 trial was confirmed objective response; efficacy analyses included patients from phase 1 and phase 2. Duration of response, progression-free survival, and safety were secondary end points in phase 2.
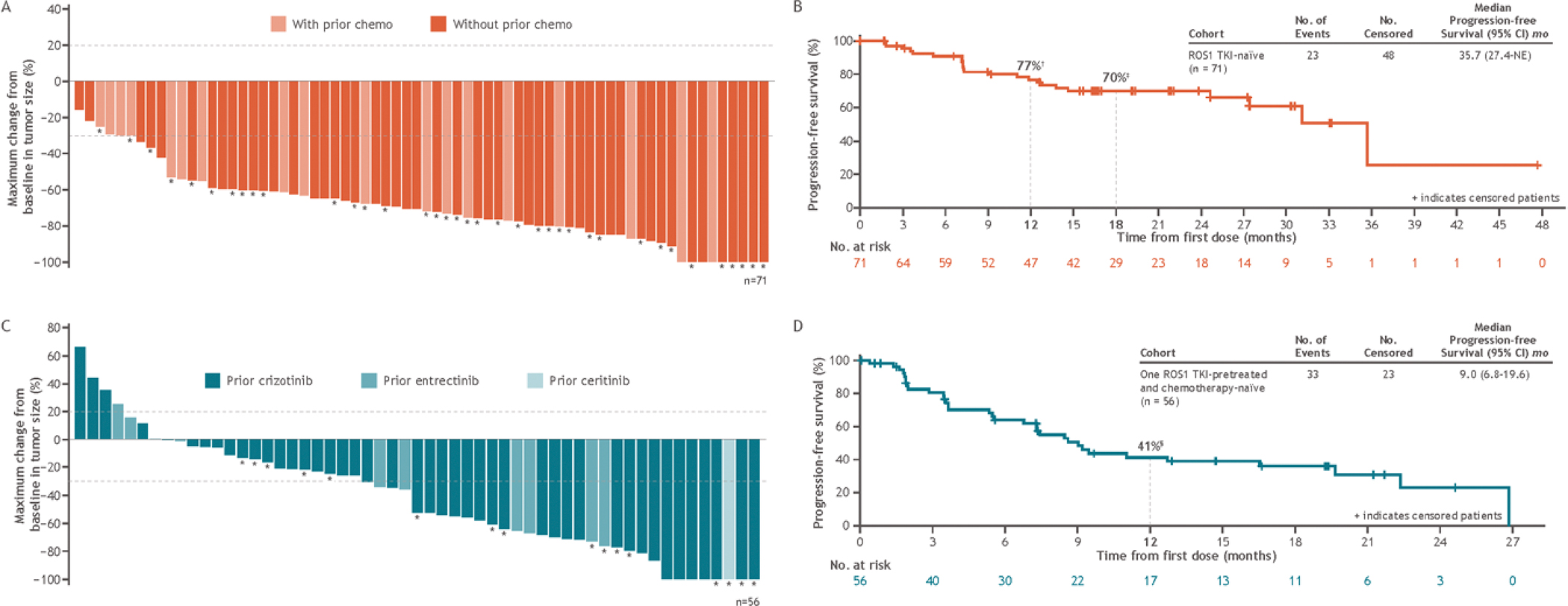
Results: On the basis of results from the phase 1 trial, the recommended phase 2 dose of repotrectinib was 160 mg daily for 14 days, followed by 160 mg twice daily. Response occurred in 56 of the 71 patients (79%; 95% confidence interval [CI], 68 to 88) with ROS1 fusion-positive NSCLC who had not previously received a ROS1 TKI; the median duration of response was 34.1 months (95% CI, 25.6 to could not be estimated), and median progression-free survival was 35.7 months (95% CI, 27.4 to could not be estimated). Response occurred in 21 of the 56 patients (38%; 95% CI, 25 to 52) with ROS1 fusion-positive NSCLC who had previously received one ROS1 TKI and had never received chemotherapy; the median duration of response was 14.8 months (95% CI, 7.6 to could not be estimated), and median progression-free survival was 9.0 months (95% CI, 6.8 to 19.6). Ten of the 17 patients (59%; 95% CI, 33 to 82) with the ROS1 G2032R mutation had a response. A total of 426 patients received the phase 2 dose; the most common treatment-related adverse events were dizziness (in 58% of the patients), dysgeusia (in 50%), and paresthesia (in 30%), and 3% discontinued repotrectinib owing to treatment-related adverse events.
Conclusions: Repotrectinib had durable clinical activity in patients with ROS1 fusion-positive NSCLC, regardless of whether they had previously received a ROS1 TKI. Adverse events were mainly of low grade and compatible with long-term administration. (Funded by Turning Point Therapeutics, a wholly owned subsidiary of Bristol Myers Squibb; TRIDENT-1 ClinicalTrials.gov number, NCT03093116.).
Copyright © 2024 Massachusetts Medical Society.
Figures
Comment in
-
ROS1 fusion-positive non-small cell lung cancer-repotrectinib as a new treatment option.Transl Cancer Res. 2025 Jun 30;14(6):3272-3276. doi: 10.21037/tcr-2025-263. Epub 2025 Jun 18. Transl Cancer Res. 2025. PMID: 40687251 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical