

Low-Dose Radiation Yields Lower Rates of Pathologic Response in Esophageal Cancer Patients
- PMID: 38198002
- PMCID: PMC10908612
- DOI: 10.1245/s10434-023-14810-8
Low-Dose Radiation Yields Lower Rates of Pathologic Response in Esophageal Cancer Patients
Abstract
Background: Although neoadjuvant chemoradiation (nCRT) followed by surgery is standard treatment for locally advanced esophageal or gastroesophageal junction (E/GEJ) cancer, the optimal radiation dose is still under debate.
Objective: The aim of this study was to assess the impact of different preoperative radiation doses (41.4 Gy, 45 Gy or 50.4 Gy) on pathologic response and survival in E/GEJ cancer patients.
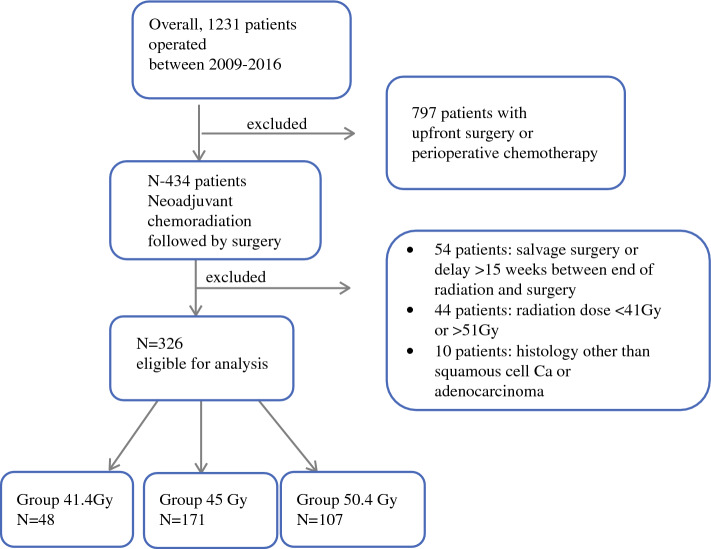
Methods: All consecutive patients with E/GEJ tumors, treated with curative intent between January 2009 and December 2016 in two referral centers were divided into three groups (41.4 Gy, 45 Gy and 50.4 Gy) according to the dose of preoperative radiotherapy. Pathologic complete response (pCR) rates, postoperative morbidity, overall survival (OS) and disease-free survival (DFS) were compared among the three groups, with separate analyses for adenocarcinoma (AC) and squamous cell carcinoma (SCC).
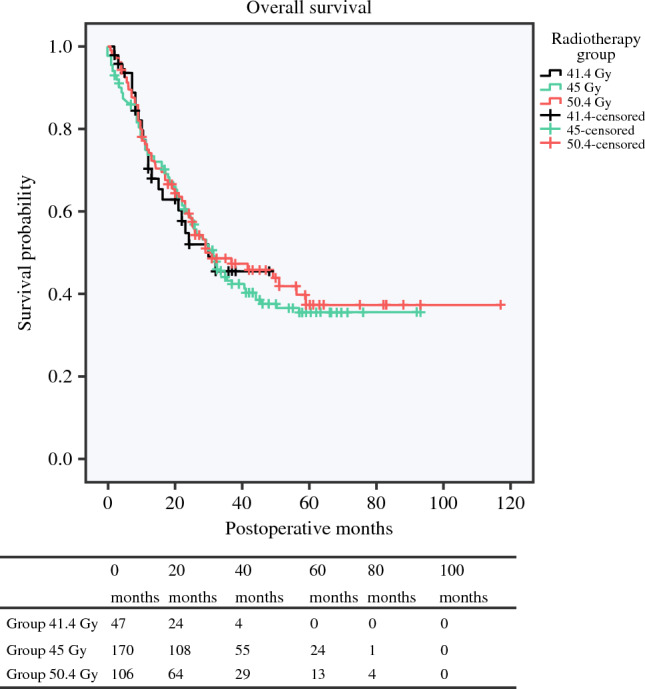
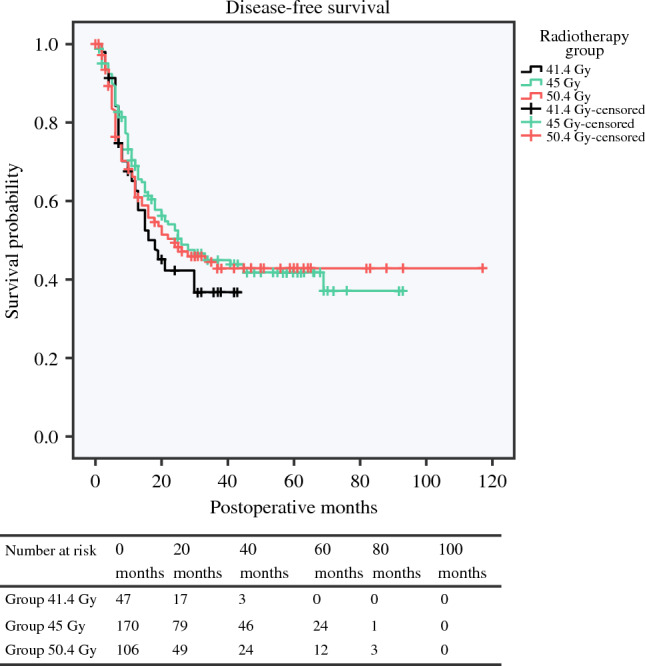
Results: From the 326 patients analyzed, 48 were included in the 41.4 Gy group (14.7%), 171 in the 45 Gy group (52.5%) and 107 in the 50.4 Gy group (32.8%). Postoperative complication rates were comparable (p = 0.399). A pCR was observed in 15%, 30%, and 34% of patients in the 41.4 Gy, 45 Gy and 50.4 Gy groups, respectively (p = 0.047). A 50.4 Gy dose was independently associated with pCR (odds ratio 2.78, 95% confidence interval 1.10-7.99) in multivariate analysis. Within AC patients, pCR was observed in 6.2% of patients in the 41.4 Gy group, 29.2% of patients in the 45 Gy group, and 22.7% of patients in the 50.4 Gy group (p = 0.035). No OS or DFS differences were observed.
Conclusions: A pCR was less common after a preoperative radiation dose of 41.4 Gy in AC patients. Radiation dose had no impact on postoperative morbidity, long-term survival, and recurrence.
Keywords: Esophageal cancer; Neoadjuvant treatment; Pathologic response; Rradiotherapy; Survival.
© 2024. The Author(s).
Conflict of interest statement
Guillaume Piessen has received consulting fees from Nestlé, BMS, and MSD, and travel expenses from Medtronic. Styliani Mantziari, Hugo Teixeira Farinha, Marguerite Messier, Michael Winiker, Pierre Allemann, Esat Mahmut Ozsahin, Nicolas Demartines, and Markus Schäfer have no conflicts of interest to declare in relation to this work.
Figures
References
-
- Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948–1957. doi: 10.1016/S0140-6736(18)32557-1. - DOI - PubMed
-
- Klevebro F, Alexandersson von Dobeln G, Wang N, et al. A randomized clinical trial of neoadjuvant chemotherapy versus neoadjuvant chemoradiotherapy for cancer of the oesophagus or gastro-oesophageal junction. Ann Oncol. 2016;27(4):660-7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
