

Cumulative Update of a Systematic Overview Evaluating Interventions Addressing Polypharmacy
- PMID: 38198136
- PMCID: PMC10782233
- DOI: 10.1001/jamanetworkopen.2023.50963
Cumulative Update of a Systematic Overview Evaluating Interventions Addressing Polypharmacy
Abstract
Importance: Polypharmacy is associated with mortality, falls, hospitalizations, and functional and cognitive decline. The study of polypharmacy-related interventions has increased substantially, prompting the need for an updated, more focused systematic overview.
Objective: To systematically evaluate and summarize evidence across multiple systematic reviews (SRs) examining interventions addressing polypharmacy.
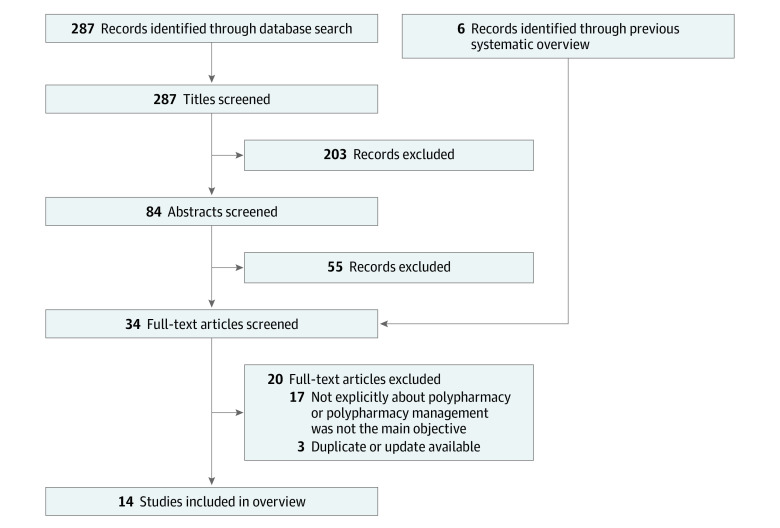
Evidence review: A search was conducted of MEDLINE, the Cochrane Database of Systematic Reviews, and the Database of Abstracts of Reviews of Effects for articles published from January 2017-October 2022, as well as those identified in a previous overview (January 2004-February 2017). Systematic reviews were included regardless of study design, setting, or outcome. The evidence was summarized by 4 categories: (1) medication-related process outcomes (eg, potentially inappropriate medication [PIM] and potential prescribing omission reductions), (2) clinical and functional outcomes, (3) health care use and economic outcomes, and (4) acceptability of the intervention.
Findings: Fourteen SRs were identified (3 from the previous overview), 7 of which included meta-analyses, representing 179 unique published studies. Nine SRs examined medication-related process outcomes (low to very low evidence quality). Systematic reviews using pooled analyses found significant reductions in the number of PIMs, potential prescribing omissions, and total number of medications, and improvements in medication appropriateness. Twelve SRs examined clinical and functional outcomes (very low to moderate evidence quality). Five SRs examined mortality; all mortality meta-analyses were null, but studies with longer follow-up periods found greater reductions in mortality. Five SRs examined falls incidence; results were predominantly null save for a meta-analysis in which PIMs were discontinued. Of the 8 SRs examining quality of life, most (7) found predominantly null effects. Ten SRs examined hospitalizations and readmissions (very low to moderate evidence quality) and 4 examined emergency department visits (very low to low evidence quality). One SR found significant reductions in hospitalizations and readmissions among higher-intensity medication reviews with face-to-face patient components. Another meta-analysis found a null effect. Of the 7 SRs without meta-analyses for hospitalizations and readmissions, all had predominantly null results. Two of 4 SRs found reductions in emergency department visits. Two SRs examined acceptability (very low evidence quality), finding wide variation in the adoption of polypharmacy-related interventions.
Conclusions and relevance: This updated systematic overview noted little evidence of an association between polypharmacy-related interventions and reduced important clinical and health care use outcomes. More evidence is needed regarding which interventions are most useful and which populations would benefit most.
Conflict of interest statement
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
