

Rethinking False Positive Exercise Electrocardiographic Stress Tests by Assessing Coronary Microvascular Function
- PMID: 38199706
- PMCID: PMC10790243
- DOI: 10.1016/j.jacc.2023.10.034
Rethinking False Positive Exercise Electrocardiographic Stress Tests by Assessing Coronary Microvascular Function
Abstract
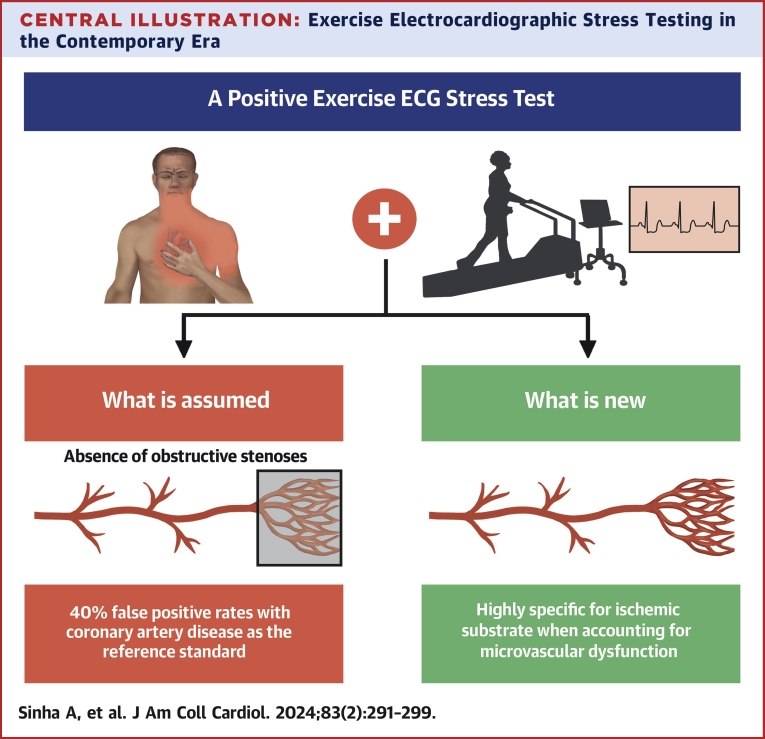
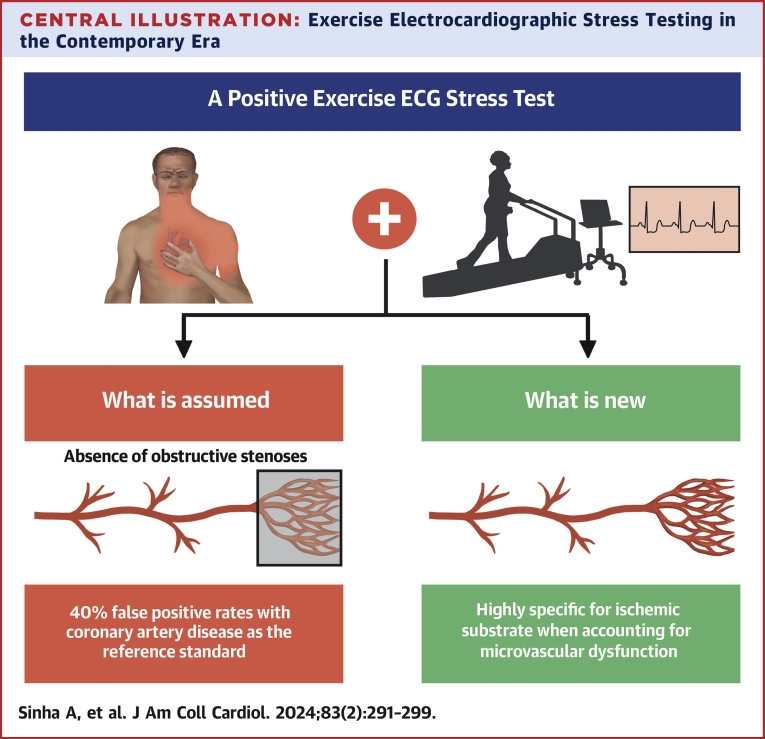
Background: Exercise electrocardiographic stress testing (EST) has historically been validated against the demonstration of obstructive coronary artery disease. However, myocardial ischemia can occur because of coronary microvascular dysfunction (CMD) in the absence of obstructive coronary artery disease.
Objectives: The aim of this study was to assess the specificity of EST to detect an ischemic substrate against the reference standard of coronary endothelium-independent and endothelium-dependent microvascular function in patients with angina with nonobstructive coronary arteries (ANOCA).
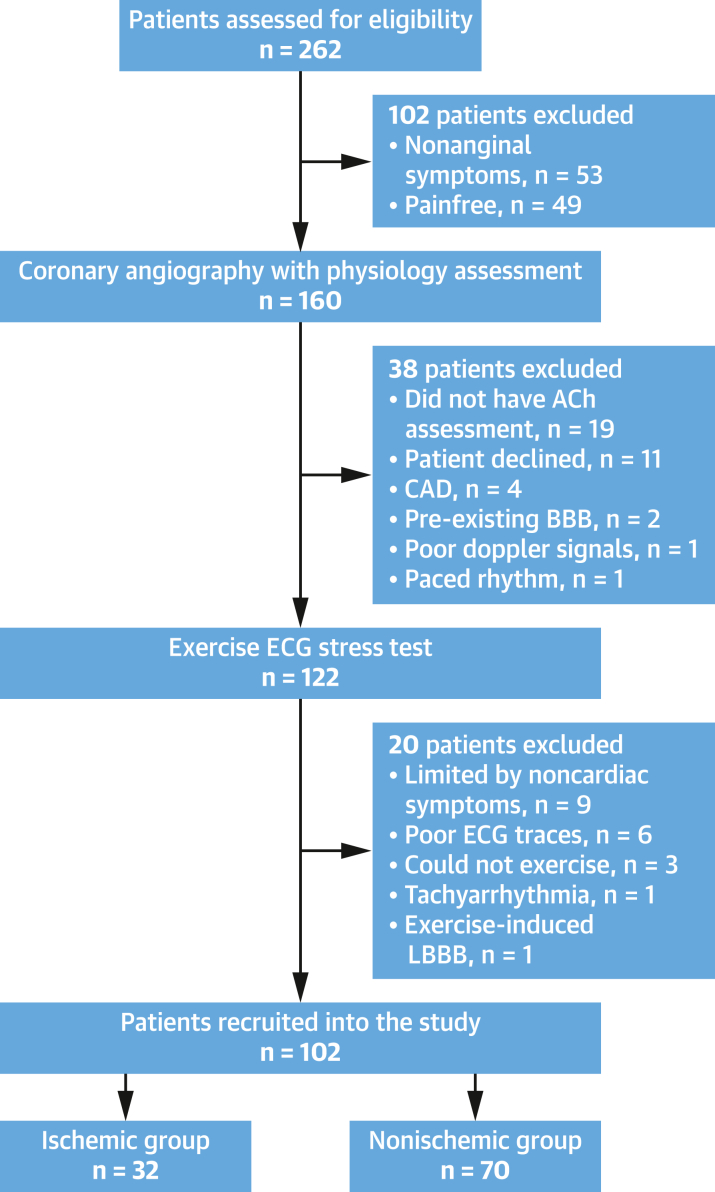
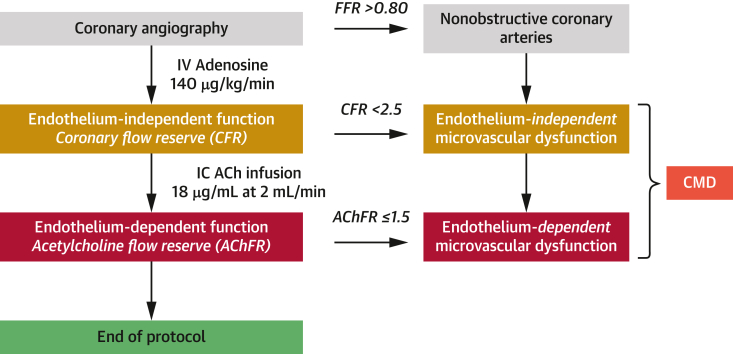
Methods: Patients with ANOCA underwent invasive coronary physiological assessment using adenosine and acetylcholine. CMD was defined as impaired endothelium-independent and/or endothelium-dependent function. EST was performed using a standard Bruce treadmill protocol, with ischemia defined as the appearance of ≥0.1-mV ST-segment depression 80 ms from the J-point on electrocardiography. The study was powered to detect specificity of ≥91%.
Results: A total of 102 patients were enrolled (65% women, mean age 60 ± 8 years). Thirty-two patients developed ischemia (ischemic group) during EST, whereas 70 patients did not (nonischemic group); both groups were phenotypically similar. Ischemia during EST was 100% specific for CMD. Acetylcholine flow reserve was the strongest predictor of ischemia during exercise. Using endothelium-independent and endothelium-dependent microvascular dysfunction as the reference standard, the false positive rate of EST dropped to 0%.
Conclusions: In patients with ANOCA, ischemia on EST was highly specific of an underlying ischemic substrate. These findings challenge the traditional belief that EST has a high false positive rate.
Keywords: acetylcholine flow reserve; coronary flow reserve; coronary microvascular dysfunction; coronary physiological assessment; exercise stress test; false positive rate.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work is supported by grants from the Medical Research Council (MR/T029390/1), the British Heart Foundation (FS/16/49/32320), and the UK National Institute for Health Research (through the Biomedical Research Center award to King’s College London and Guy’s and St. Thomas’ Hospital). Prof Shah is supported by the British Heart Foundation (CH/1999001/11735). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Clinical Utility of the Humble Exercise ECG Stress Test.J Am Coll Cardiol. 2024 Jan 16;83(2):300-302. doi: 10.1016/j.jacc.2023.10.036. J Am Coll Cardiol. 2024. PMID: 38199707 No abstract available.
References
-
- Knuuti J., Wijns W., Saraste A., et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41:407–477. - PubMed
-
- Perera D., Berry C., Hoole S.P., et al. Invasive coronary physiology in patients with angina and non-obstructive coronary artery disease: a consensus document from the coronary microvascular dysfunction workstream of the British Heart Foundation/National Institute for Health Research Partnership. Heart. 2023;109:88–95. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
