

Clinical and preclinical evidence that angiotensin-converting enzyme inhibitors and angiotensin receptor blockers prevent diabetic peripheral neuropathy
- PMID: 38200077
- PMCID: PMC10781693
- DOI: 10.1038/s41598-024-51572-z
Clinical and preclinical evidence that angiotensin-converting enzyme inhibitors and angiotensin receptor blockers prevent diabetic peripheral neuropathy
Abstract
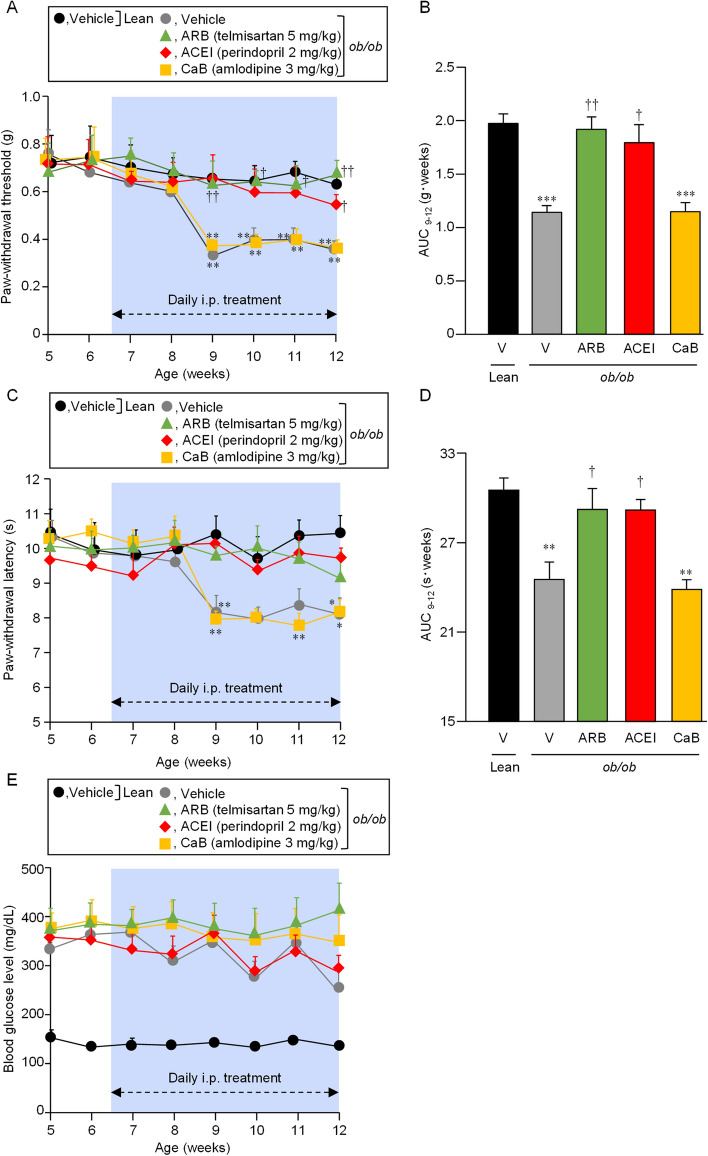
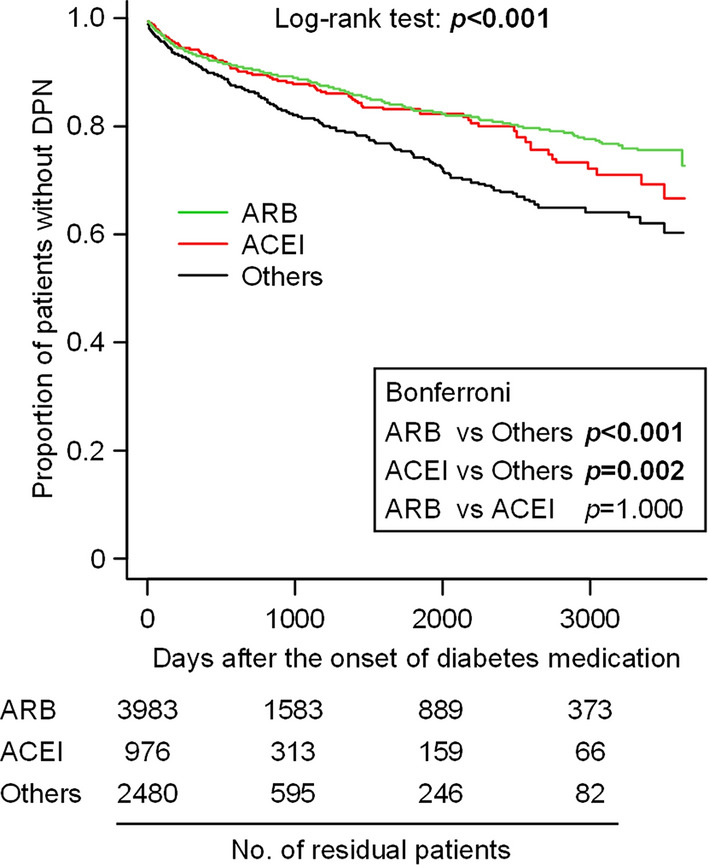
Given possible involvement of the central and peripheral angiotensin system in pain processing, we conducted clinical and preclinical studies to test whether pharmacological inhibition of the angiotensin system would prevent diabetic peripheral neuropathy (DPN) accompanying type 2 diabetes mellitus (T2DM). In the preclinical study, the nociceptive sensitivity was determined in leptin-deficient ob/ob mice, a T2DM model. A clinical retrospective cohort study was conducted, using the medical records of T2DM patients receiving antihypertensives at three hospitals for nearly a decade. In the ob/ob mice, daily treatment with perindopril, an angiotensin-converting enzyme inhibitor (ACEI), or telmisartan, an angiotensin receptor blocker (ARB), but not amlodipine, an L-type calcium channel blocker (CaB), significantly inhibited DPN development without affecting the hyperglycemia. In the clinical study, the enrolled 7464 patients were divided into three groups receiving ACEIs, ARBs and the others (non-ACEI, non-ARB antihypertensives). Bonferroni's test indicated significantly later DPN development in the ARB and ACEI groups than the others group. The multivariate Cox proportional analysis detected significant negative association of the prescription of ACEIs or ARBs and β-blockers, but not CaBs or diuretics, with DPN development. Thus, our study suggests that pharmacological inhibition of the angiotensin system is beneficial to prevent DPN accompanying T2DM.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
EVALUATING THE PRESCRIPTION OF ANGIOTENSIN-CONVERTING ENZYME INHIBITORS OR RECEPTOR BLOCKERS IN PATIENTS WITH DIABETES IN JORDAN.Endocr Pract. 2017 Nov;23(11):1289-1296. doi: 10.4158/EP171917.OR. Epub 2017 Aug 17. Endocr Pract. 2017. PMID: 28816537
-
Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers reduced dementia risk in patients with diabetes mellitus and hypertension.Int J Cardiol. 2016 Oct 1;220:462-6. doi: 10.1016/j.ijcard.2016.06.215. Epub 2016 Jun 27. Int J Cardiol. 2016. PMID: 27390970
-
Angiotensin-converting enzyme inhibitors, angiotensin-II-receptor antagonists and angiotensin-receptor blocker/neprilysin inhibitor utilization in heart failure patients: Sub-analysis of a nation-wide population-based study in the Czech Republic.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2022 Sep;166(3):322-327. doi: 10.5507/bp.2021.035. Epub 2021 Jun 4. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2022. PMID: 34092792
-
Role of antihypertensive therapy with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers in combination with calcium channel blockers for stroke prevention.J Am Pharm Assoc (2003). 2010 Sep-Oct;50(5):e116-25. doi: 10.1331/JAPhA.2010.09234. J Am Pharm Assoc (2003). 2010. PMID: 20833609 Review.
-
A review of chemical therapies for treating diabetic hypertension.Expert Opin Pharmacother. 2017 Jun;18(9):909-923. doi: 10.1080/14656566.2017.1328054. Epub 2017 May 16. Expert Opin Pharmacother. 2017. PMID: 28480805 Review.
Cited by
-
Cardiovascular autonomic neuropathy in diabetes: an update with a focus on management.Diabetologia. 2024 Dec;67(12):2611-2625. doi: 10.1007/s00125-024-06242-0. Epub 2024 Aug 9. Diabetologia. 2024. PMID: 39120767 Free PMC article. Review.
-
Combination therapy is it in the future for successfully treating peripheral diabetic neuropathy?Front Endocrinol (Lausanne). 2024 May 15;15:1357859. doi: 10.3389/fendo.2024.1357859. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38812811 Free PMC article. Review.
-
Taxane-Associated Acute Pain Syndrome: a Review of its Features and Management.Curr Treat Options Oncol. 2025 Mar;26(3):187-196. doi: 10.1007/s11864-025-01302-y. Epub 2025 Feb 28. Curr Treat Options Oncol. 2025. PMID: 40019675 Review.
-
Current understanding of the link between angiotensin-converting enzyme and pain perception.Drug Discov Today. 2024 Sep;29(9):104089. doi: 10.1016/j.drudis.2024.104089. Epub 2024 Jul 6. Drug Discov Today. 2024. PMID: 38977123 Review.
References
-
- Banerjee D, et al. Management of hypertension and renin-angiotensin-aldosterone system blockade in adults with diabetic kidney disease: Association of British clinical diabetologists and the renal association UK guideline update 2021. BMC Nephrol. 2022;23:9. doi: 10.1186/s12882-021-02587-5. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
