

The artificial intelligence-based model ANORAK improves histopathological grading of lung adenocarcinoma
- PMID: 38200244
- PMCID: PMC10899116
- DOI: 10.1038/s43018-023-00694-w
The artificial intelligence-based model ANORAK improves histopathological grading of lung adenocarcinoma
Abstract
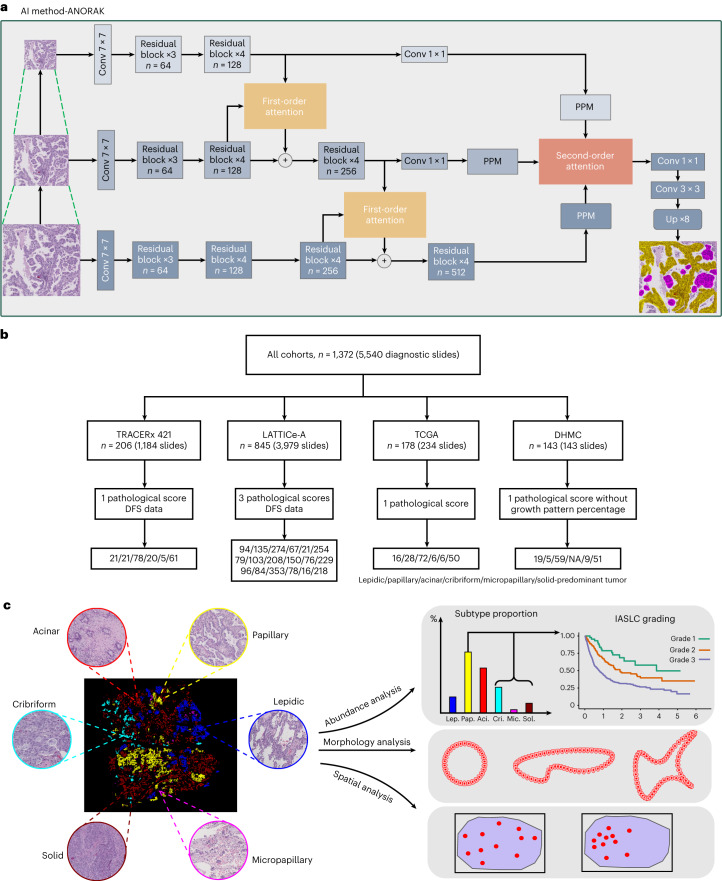
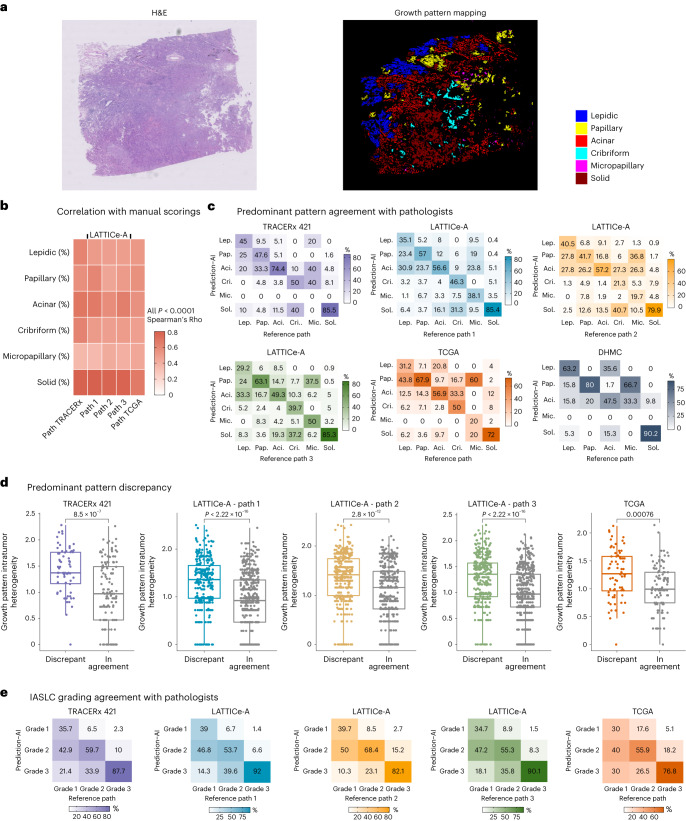
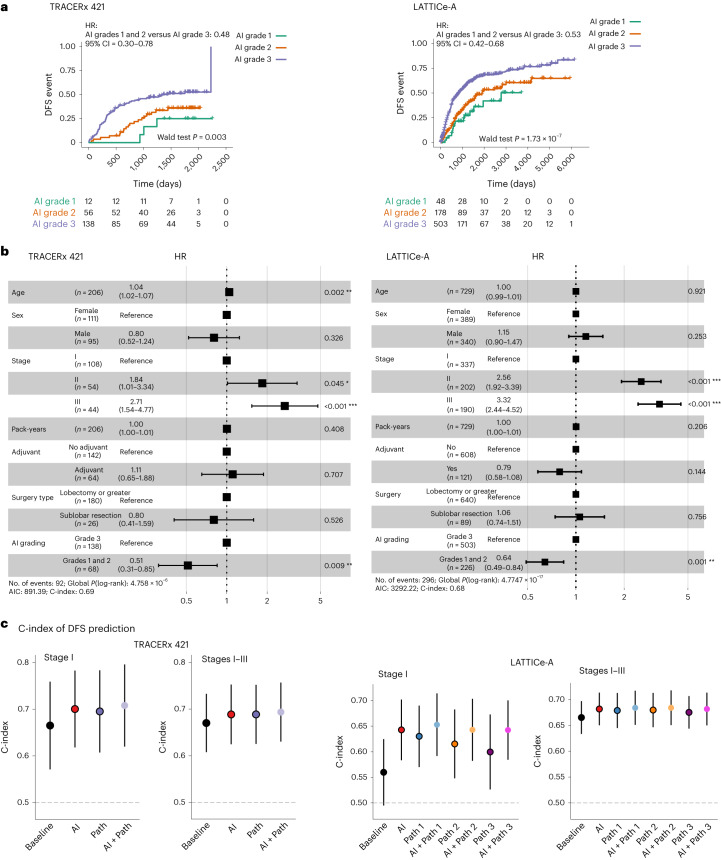
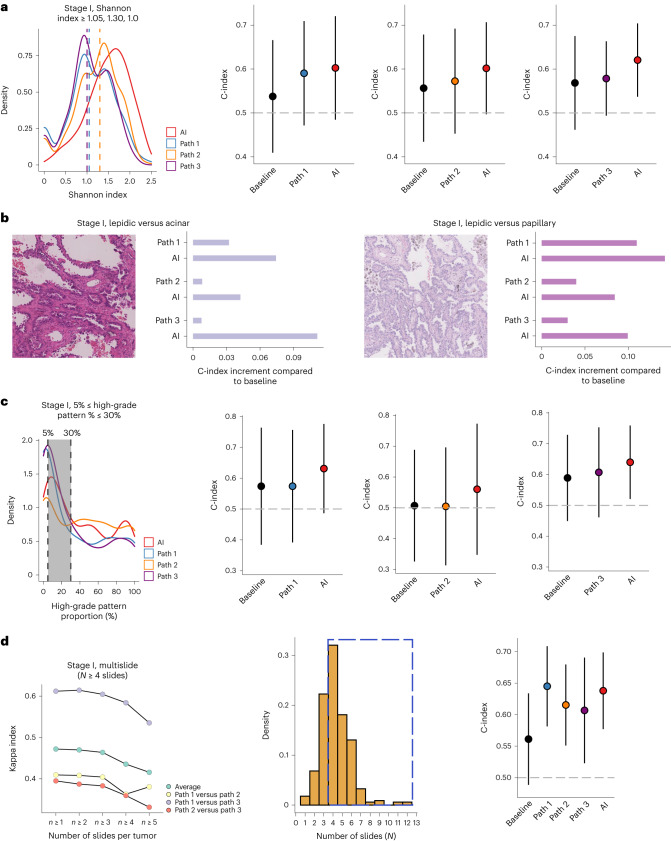
The introduction of the International Association for the Study of Lung Cancer grading system has furthered interest in histopathological grading for risk stratification in lung adenocarcinoma. Complex morphology and high intratumoral heterogeneity present challenges to pathologists, prompting the development of artificial intelligence (AI) methods. Here we developed ANORAK (pyrAmid pooliNg crOss stReam Attention networK), encoding multiresolution inputs with an attention mechanism, to delineate growth patterns from hematoxylin and eosin-stained slides. In 1,372 lung adenocarcinomas across four independent cohorts, AI-based grading was prognostic of disease-free survival, and further assisted pathologists by consistently improving prognostication in stage I tumors. Tumors with discrepant patterns between AI and pathologists had notably higher intratumoral heterogeneity. Furthermore, ANORAK facilitates the morphological and spatial assessment of the acinar pattern, capturing acinus variations with pattern transition. Collectively, our AI method enabled the precision quantification and morphology investigation of growth patterns, reflecting intratumoral histological transitions in lung adenocarcinoma.
Trial registration: ClinicalTrials.gov NCT01888601.
© 2024. The Author(s).
Conflict of interest statement
S.V. is a coinventor to a patent of methods for detecting molecules in a sample (patent no. 10578620). A.H. has received fees from Abbvie, Almirall, Boehringer Ingelheim, Clovis Oncology, Ipsen, Takeda Pharmaceuticals, AstraZeneca, Daiichi Sankyo, Merck Serono, Merck/MSD, UCB, Kyowa Kirin, Servier, Sobi, Pfizer and Roche for delivering general education and training in clinical trials; has received fees for member of independent data monitoring committees for Roche-sponsored clinical trials and academic projects on real-world evidence or tumor-agnostic therapies coordinated by Roche; he has been paid honoraria for speaking at Roche-funded conferences (on real-world data); he has an academic collaboration with Navio and is an unpaid member of their advisory board; he is an investigator for an academic study (SUMMIT) sponsored by UCL, which is funded by GRAIL; he has received one honorarium for an advisory board meeting for GRAIL; he has received a consulting fee from Evidera (for one GRAIL-initiated project); and he has previously owned shares in Illumina and Thermo Fisher Scientific (sold in 2020); he is on the scientific advisory board for Adela Bio and has received no payments or honoraria for this, although he has share options available. A.G.N. reports personal fees from Merck, Boehringer Ingelheim, Novartis, AstraZeneca, Bristol Myers Squibb, Roche, Abbvie, Oncologica, Uptodate, the European Society of Oncology, Takeda Pharmaceuticals, Sanofi and Liberium, as well as personal fees and grants from Pfizer. M.J-H. is a Cancer Research UK Career Establishment Awardee and has received funding from Cancer Research UK, the International Association for the Study of Lung Cancer and International Lung Cancer Foundation, the Lung Cancer Research Foundation, the Rosetrees Trust, UK and Ireland Neuroendocrine Tumour Society, the National Institute for Health Research (NIHR) and the NIHR UCLH Biomedical Research Centre. M.J-H. has consulted for, and is a member of, the Achilles Therapeutics Scientific advisory board and steering committee, has received speaker honoraria from Pfizer, Astex Pharmaceuticals and Oslo Cancer Cluster, and holds a patent (no. PCT/US2017/028013) relating to methods for lung cancer detection. C.S. acknowledges grant support from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Pfizer, Roche-Ventana, Invitae (previously Archer Dx, collaboration in minimal residual disease sequencing technologies) and Ono Pharmaceutical. He is an AstraZeneca advisory board member and chief investigator for the AZ MeRmaiD 1 and 2 clinical trials; he is also co-chief investigator of the NHS Galleri trial funded by GRAIL and a paid member of GRAIL’s scientific advisory board. He receives consultant fees from Achilles Therapeutics (scientific advisory board member), Bicycle Therapeutics (scientific advisory board), Genentech, Medicxi, Roche Innovation Centre-Shanghai, Metabomed (until July 2022) and the Sarah Cannon Research Institute. C.S. has received honoraria from Amgen, AstraZeneca, Pfizer, Novartis, GlaxoSmithKline, MSD, Bristol Myers Squibb, Illumina and Roche-Ventana. C.S. had stock options in Apogen Biotechnologies and GRAIL until June 2021; he currently has stock options in Epic Bioscience, Bicycle Therapeutics; he has stock options and is a cofounder of Achilles Therapeutics. C.S. holds patents relating to assay technology to detect tumor recurrence (no. PCT/GB2017/053289), target neoantigens (no. PCT/EP2016/059401), identify patent response to immune checkpoint blockade (no. PCT/EP2016/071471), determine HLA loss of heterozygosity (no. PCT/GB2018/052004), predict survival rates of patients with cancer (no. PCT/GB2020/050221) and identify patients who respond to cancer treatment (no. PCT/GB2018/051912), as well as a US patent related to detecting tumor mutations (no. PCT/US2017/28013) and methods for lung cancer detection (no. US20190106751A1), and both European and US patents related to identifying insertion and deletion mutation targets (no. PCT/GB2018/051892). Y.Y. has received speaker’s bureau honoraria from Roche and consulted for Merck. D.A.M. reports speaker fees from Eli Lilly, AstraZeneca and Takeda Pharmaceuticals, consultancy fees from AstraZeneca, Thermo Fisher Scientific, Takeda Pharmaceuticals, Amgen, Janssen, MIM Software, Bristol Myers Squibb and Eli Lilly, and has received educational support from Takeda Pharmaceuticals and Amgen. All other authors declare no competing interests.
Figures








References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
