Association between spinal manipulative therapy and lumbar spine reoperation after discectomy: a retrospective cohort study
- PMID: 38200469
- PMCID: PMC10777506
- DOI: 10.1186/s12891-024-07166-x
Association between spinal manipulative therapy and lumbar spine reoperation after discectomy: a retrospective cohort study
Abstract
Background: Patients who undergo lumbar discectomy may experience ongoing lumbosacral radiculopathy (LSR) and seek spinal manipulative therapy (SMT) to manage these symptoms. We hypothesized that adults receiving SMT for LSR at least one year following lumbar discectomy would be less likely to undergo lumbar spine reoperation compared to matched controls not receiving SMT, over two years' follow-up.
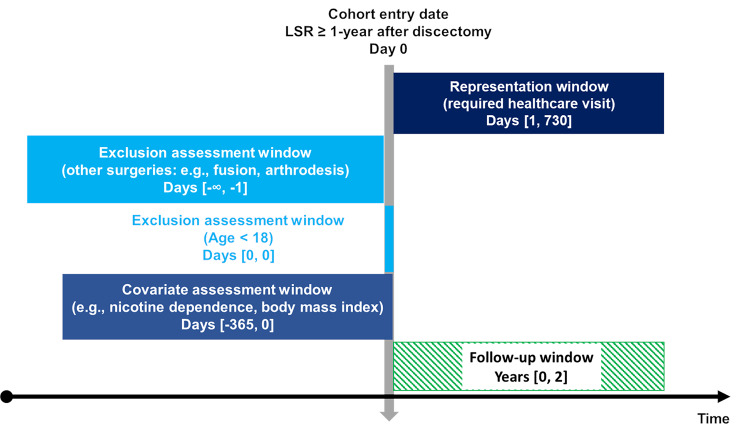
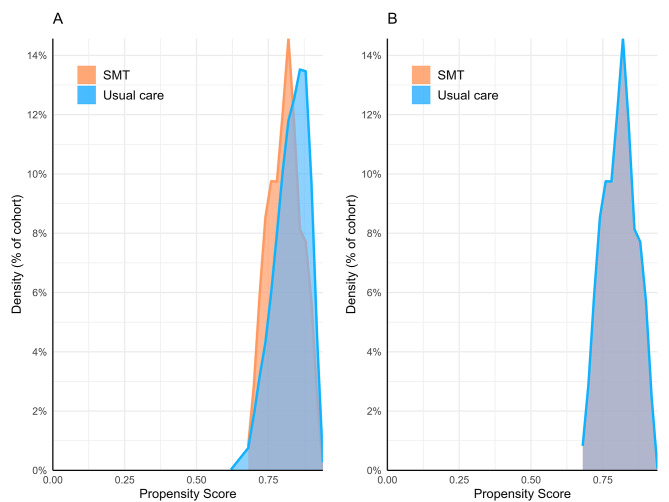
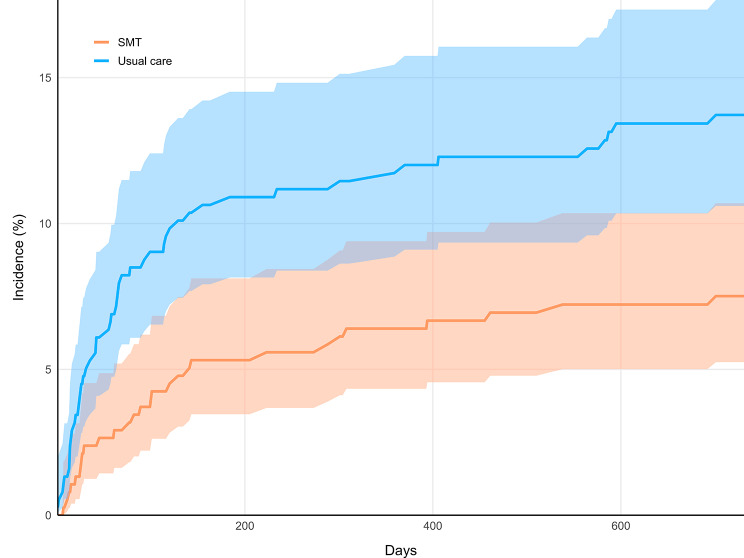
Methods: We searched a United States network of health records (TriNetX, Inc.) for adults aged ≥ 18 years with LSR and lumbar discectomy ≥ 1 year previous, without lumbar fusion or instrumentation, from 2003 to 2023. We divided patients into two cohorts: (1) chiropractic SMT, and (2) usual care without chiropractic SMT. We used propensity matching to adjust for confounding variables associated with lumbar spine reoperation (e.g., age, body mass index, nicotine dependence), calculated risk ratios (RR), with 95% confidence intervals (CIs), and explored cumulative incidence of reoperation and the number of SMT follow-up visits.
Results: Following propensity matching there were 378 patients per cohort (mean age 61 years). Lumbar spine reoperation was less frequent in the SMT cohort compared to the usual care cohort (SMT: 7%; usual care: 13%), yielding an RR (95% CIs) of 0.55 (0.35-0.85; P = 0.0062). In the SMT cohort, 72% of patients had ≥ 1 follow-up SMT visit (median = 6).
Conclusions: This study found that adults experiencing LSR at least one year after lumbar discectomy who received SMT were less likely to undergo lumbar spine reoperation compared to matched controls not receiving SMT. While these findings hold promise for clinical implications, they should be corroborated by a prospective study including measures of pain, disability, and safety to confirm their relevance. We cannot exclude the possibility that our results stem from a generalized effect of engaging with a non-surgical clinician, a factor that may extend to related contexts such as physical therapy or acupuncture.
Registration: Open Science Framework ( https://osf.io/vgrwz ).
Keywords: Chiropractic; Intervertebral disc; Lumbar vertebrae; Lumbosacral region; Spinal manipulation; Surgical decompression.
© 2024. The Author(s).
Conflict of interest statement
Dr. Trager reports he has received book royalties as the author of two texts on the topic of sciatica. The other authors declare that they have no competing interests.
Figures