

Conversion surgery for initially unresectable locally advanced pancreatic ductal adenocarcinoma after chemotherapy followed by carbon-ion radiotherapy: a case report
- PMID: 38200536
- PMCID: PMC10782725
- DOI: 10.1186/s13256-023-04311-3
Conversion surgery for initially unresectable locally advanced pancreatic ductal adenocarcinoma after chemotherapy followed by carbon-ion radiotherapy: a case report
Abstract
Background: Recent advances in chemotherapy and chemoradiotherapy have enabled conversion surgery (CS) to be performed for selected patients with initially unresectable locally advanced (LA) pancreatic ductal adenocarcinoma (PDAC). Many studies indicate CS might extend the survival of patients with initially unresectable LA PDAC. However, several clinical questions concerning CS remain, such as the optimal preoperative treatment. Carbon-ion radiotherapy (CIRT) is a unique radiotherapy that offers higher biological effectiveness than conventional radiotherapy. Here, we report a long-term survival case with initially unresectable LA PDAC who underwent CS after chemotherapy followed by CIRT.
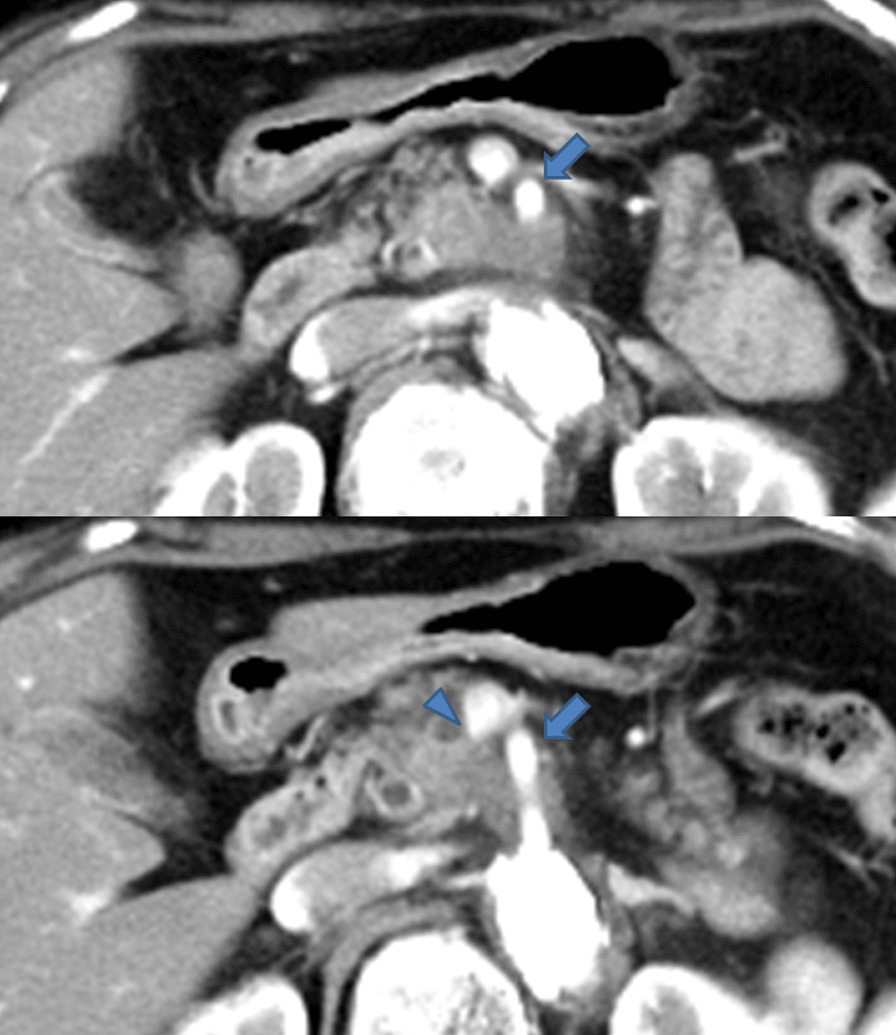
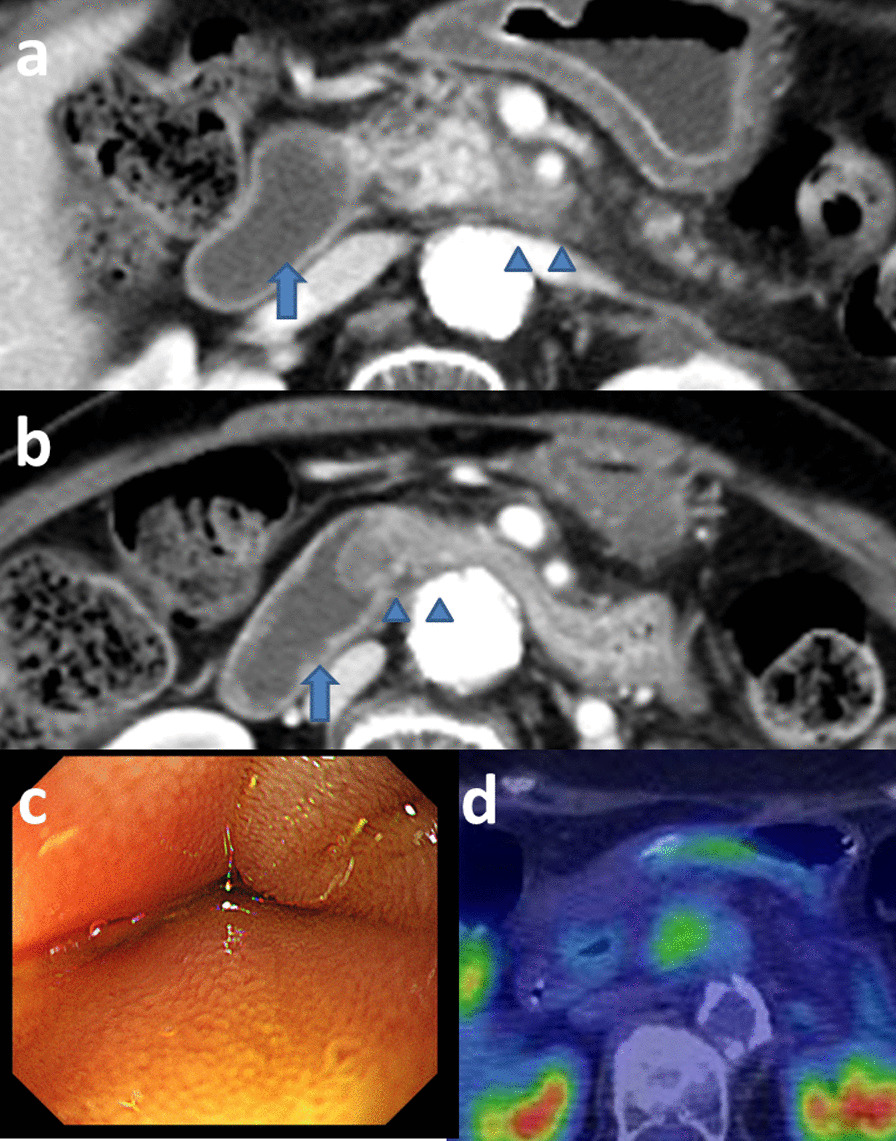
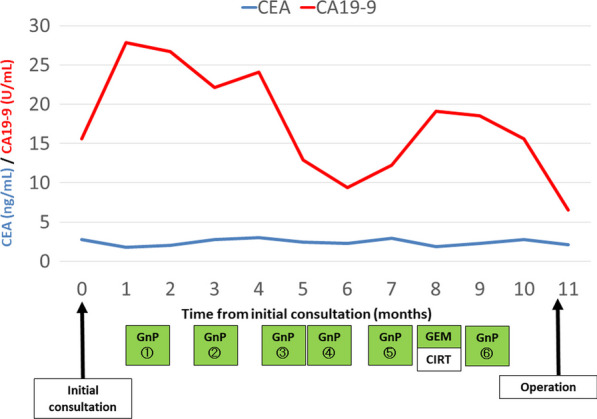
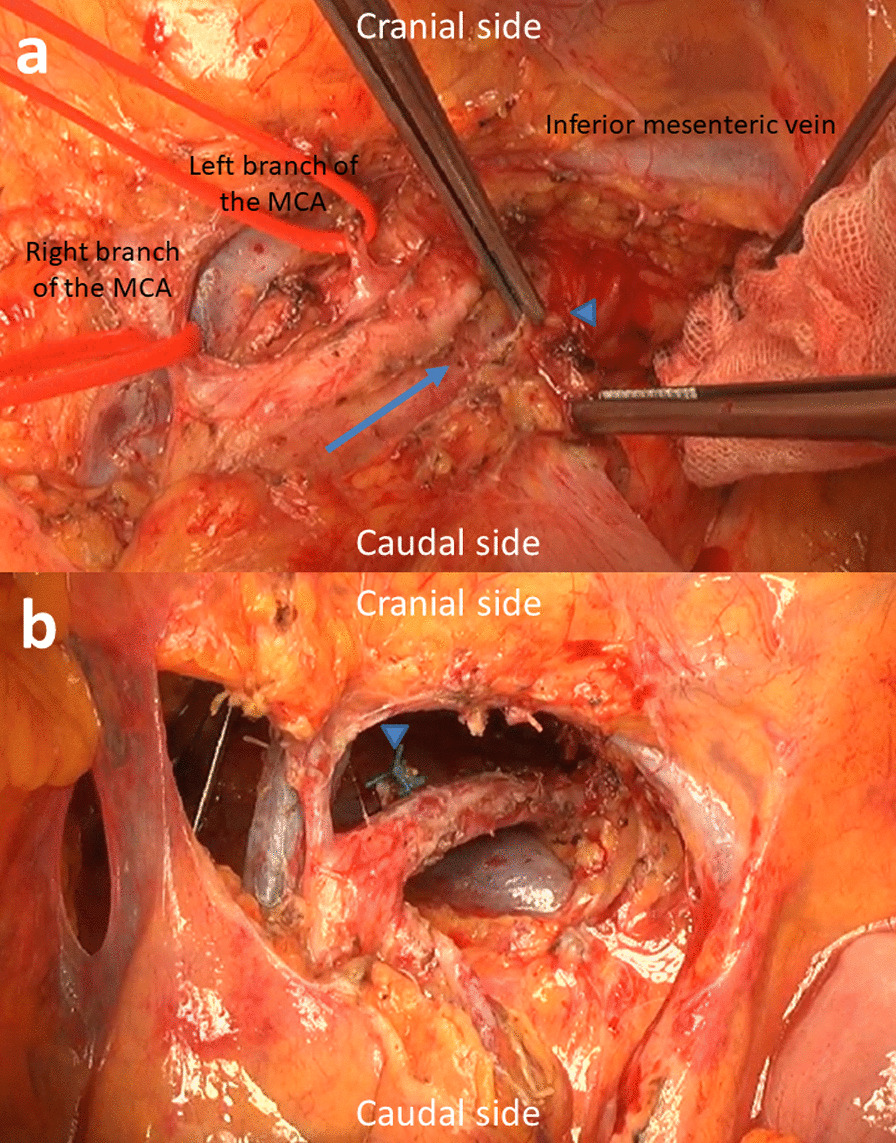
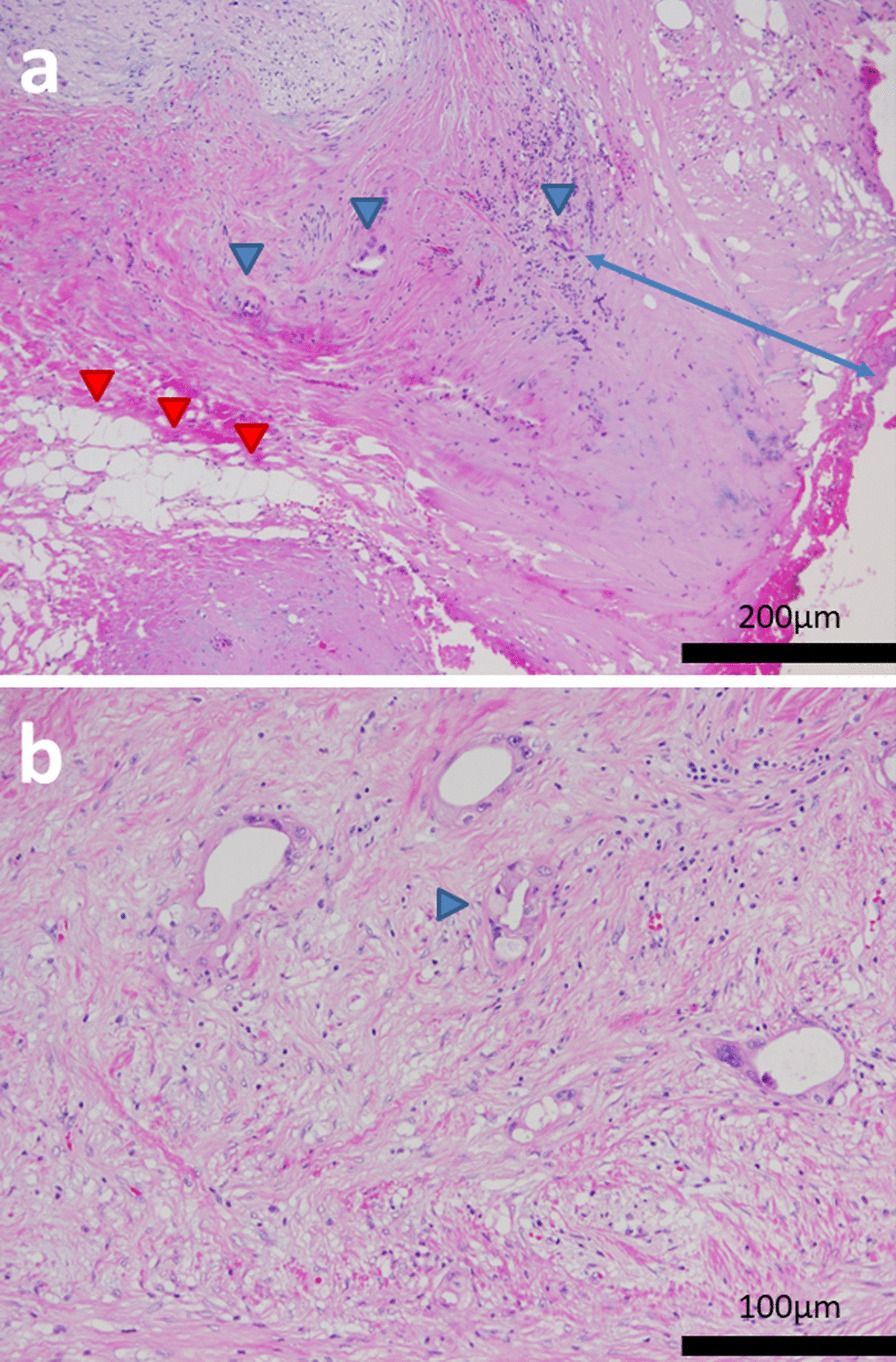
Case presentation: The patient was a 72-year-old Japanese woman with unresectable LA pancreatic head cancer with tumor contact to the superior mesenteric artery (SMA). She underwent four courses of chemotherapy (gemcitabine plus nanoparticle albumin-bound paclitaxel). However, the lesion did not shrink and tumor contact with the SMA did not improve after chemotherapy. Because the probability of achieving curative resection was judged to be low, she underwent radical dose CIRT, and chemotherapy was continued. She complained of vomiting 2 months after CIRT. Although imaging studies showed no tumor growth or metastasis, a duodenal obstruction which was speculated to be an adverse effect of CIRT was observed. She could not eat solid food and a trans-nasal feeding tube was inserted. Therapeutic intervention was required to enable enteral nutrition. We proposed several treatment options. She chose resection with the expectation of an anti-tumor effect of chemotherapy and CIRT rather than course observation with tube feeding or bypass surgery. Therefore, subtotal-stomach-preserving pancreatoduodenectomy with portal vein resection was performed as CS. Pathological examination of the resected specimen revealed an R0 resection with a histological response of Evans grade IIA. Postoperatively, she recovered uneventfully. Adjuvant chemotherapy with tegafur/gimeracil/oteracil (S1) was administrated. At the time of this report, 5 years have passed since the initial consultation and she has experienced no tumor recurrence.
Conclusions: The present case suggests that multidisciplinary treatment consisting of a combination of recent chemotherapy and CIRT may be beneficial for unresectable LA PDAC. However, further studies are required to assess the true efficacy of this treatment strategy.
Keywords: Carbon-ion radiotherapy; Conversion surgery; Pancreatic ductal adenocarcinoma.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests related to this manuscript.
Figures
References
-
- Satoi S, Yamaue H, Kato K, et al. Role of adjuvant surgery for patients with initially unresectable pancreatic cancer with a long-term favorable responses to non-surgical anti-cancer treatments: results of a project study for pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J Hepatobiliary Pancreat Sci. 2013;20:590–600. doi: 10.1007/s00534-013-0616-0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
