

Mid-Term Results of an Italian Multicentric Experience with the RoadsaverTM Dual-Layer Carotid Stent System
- PMID: 38201025
- PMCID: PMC10778716
- DOI: 10.3390/healthcare12010120
Mid-Term Results of an Italian Multicentric Experience with the RoadsaverTM Dual-Layer Carotid Stent System
Abstract
Background: Carotid artery stenting (CAS) using first-generation single-layer stents is widely accepted as a good alternative to standard carotid endarterectomy (CEA) but it is associated with worse outcomes in terms of both plaque prolapse and cerebral embolization.
Aim: To evaluate the perioperative and midterm outcomes of CAS using the new-generation RoadsaverTM dual-layer micromesh-covered carotid stent.
Methods: Herein, we present the results of an observational, retrospective, multicentric study on non-consecutive patients who underwent the CAS procedure between January 2017 and December 2022 at three Italian, high-volume vascular surgery centers. The inclusion criteria were the patients' eligibility for the CAS procedure in accordance with the current Italian guidelines, and the implantation of a Roadsaver stent. Both symptomatic and asymptomatic patients were included in the study. The patients requiring reintervention for carotid restenosis following CEA were also included. Perioperative data regarding procedural success was defined as the successful implantation of the device in the desired position, less than 30% residual stenosis, and the absence of intraoperative neurological complications. The primary outcome was any adverse cerebrovascular event such as stroke or transient ischemic attack (TIA) during the procedure and/or after discharge. The secondary outcomes were the need for further intervention, and all-cause death following procedure.
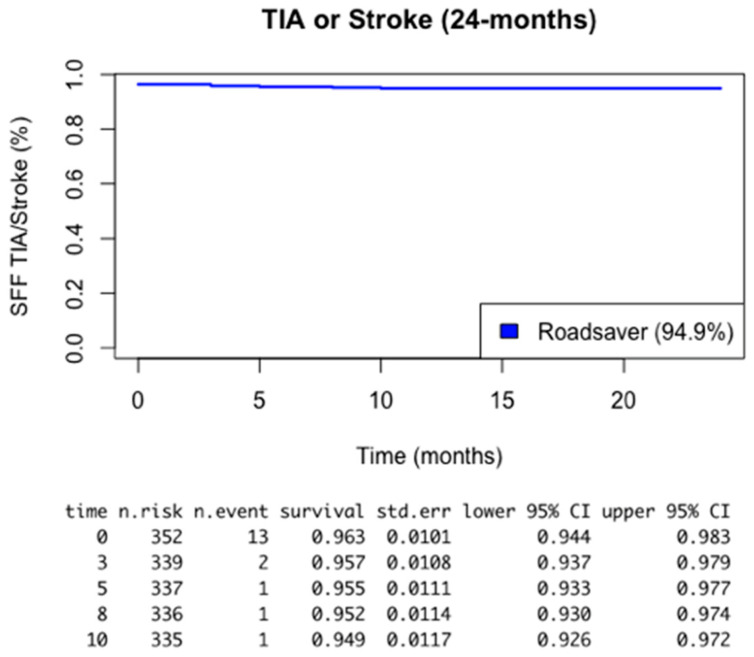
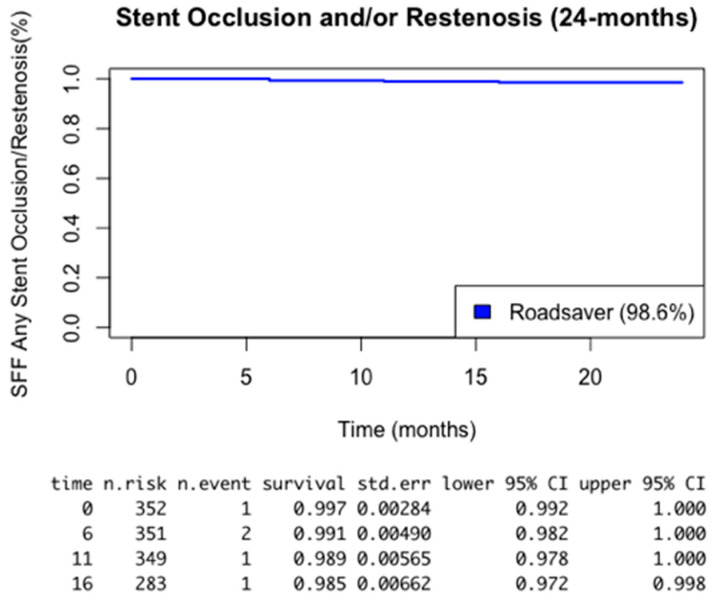
Results: Three-hundred-fifty-three (353) patients were included in our study; the mean age was 74.3 years. A total of 5.9% of the patients were symptomatic on their operated side, while 7.3% had contralateral carotid occlusion. A cerebral embolic protection device (CPD) was employed in all patients. A total of 13.3% of the patients were operated on for restenosis after CEA Technical success was achieved in 96.9% of the cases with an intraoperative report of six TIAs (1.7%) and six ipsilateral strokes (1.7%). The mean hospital stay was 1.8 days. The thirty-day follow up showed one TIA and one more stroke. At the mean 35-month follow-up time, the primary outcome was present in six patients (1.7%), where four TIAs (1.1%) and two strokes (0.5%) were reported. Restenosis occurred in five patients (1.4%). Death for any cause was reported in 11 patients (3.1%).
Conclusions: As most recent, high-quality studies show, the CAS procedure with second-generation devices such as the Roadsaver stent is safe and effective in preventing carotid-related cerebrovascular events in both symptomatic and asymptomatic patients. The intraoperative and postoperative cerebrovascular complication rate in high volume centers is very low, ensuring confidence in its employment for the CAS procedure along with a CPD as a valid alternative to CEA.
Keywords: carotid artery stenosis; carotid artery stenting; dual-layer stent; micromesh; stroke.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Hrbáč T., Fiedler J., Procházka V., Jonszta T., Roubec M., Pakizer D., Václavík D., Netuka D., Heryán T., Školoudík D. Comparison of carotid endarterectomy and repeated carotid angioplasty and stenting for in-stent restenosis (CERCAS trial): A randomised study. Stroke Vasc. Neurol. 2023;8:2075. doi: 10.1136/svn-2022-002075. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
