

Machine Learning Approach for Improved Longitudinal Prediction of Progression from Mild Cognitive Impairment to Alzheimer's Disease
- PMID: 38201322
- PMCID: PMC10795823
- DOI: 10.3390/diagnostics14010013
Machine Learning Approach for Improved Longitudinal Prediction of Progression from Mild Cognitive Impairment to Alzheimer's Disease
Abstract
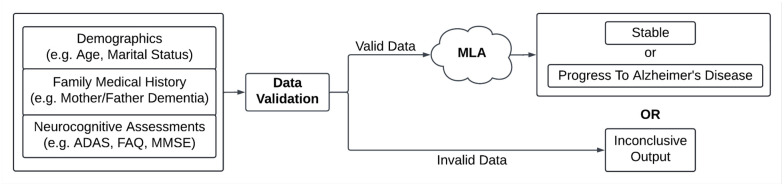
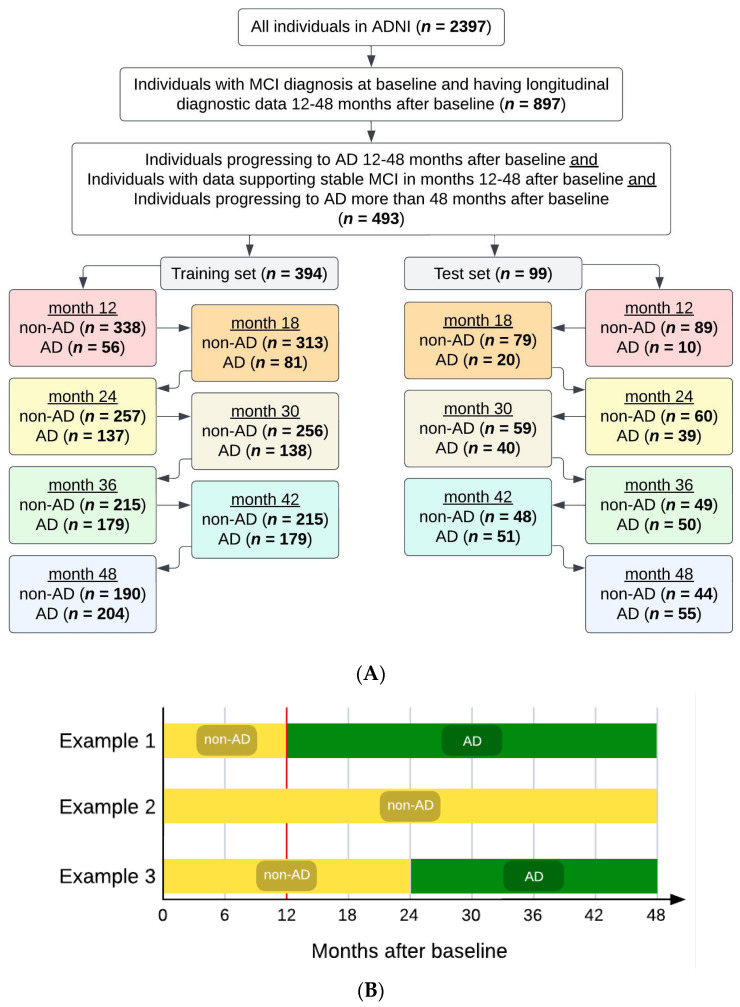
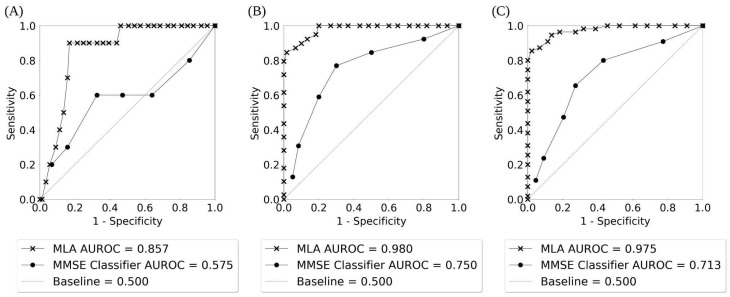
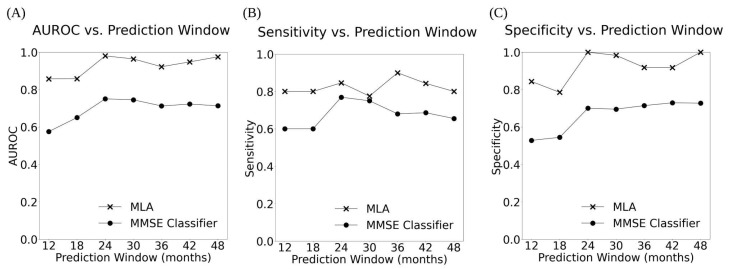
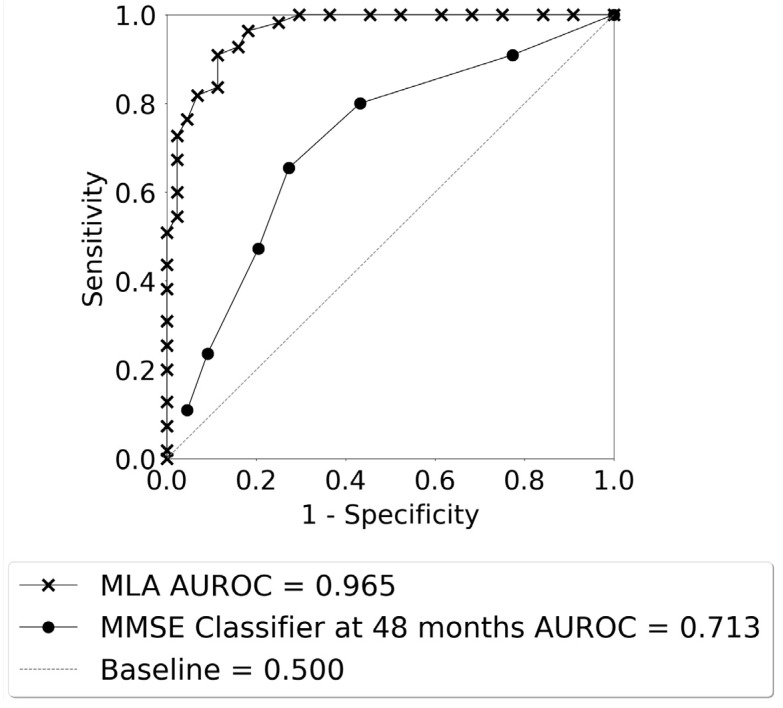
Mild cognitive impairment (MCI) is cognitive decline that can indicate future risk of Alzheimer's disease (AD). We developed and validated a machine learning algorithm (MLA), based on a gradient-boosted tree ensemble method, to analyze phenotypic data for individuals 55-88 years old (n = 493) diagnosed with MCI. Data were analyzed within multiple prediction windows and averaged to predict progression to AD within 24-48 months. The MLA outperformed the mini-mental state examination (MMSE) and three comparison models at all prediction windows on most metrics. Exceptions include sensitivity at 18 months (MLA and MMSE each achieved 0.600); and sensitivity at 30 and 42 months (MMSE marginally better). For all prediction windows, the MLA achieved AUROC ≥ 0.857 and NPV ≥ 0.800. With averaged data for the 24-48-month lookahead timeframe, the MLA outperformed MMSE on all metrics. This study demonstrates that machine learning may provide a more accurate risk assessment than the standard of care. This may facilitate care coordination, decrease healthcare expenditures, and maintain quality of life for patients at risk of progressing from MCI to AD.
Keywords: Alzheimer’s disease; disease progression; machine learning; mild cognitive impairment.
Conflict of interest statement
All authors are employees or contractors of Montera, Inc. dba Forta. Authors declare that research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Figures
Similar articles
-
ApoE4 effects on automated diagnostic classifiers for mild cognitive impairment and Alzheimer's disease.Neuroimage Clin. 2014 Jan 4;4:461-72. doi: 10.1016/j.nicl.2013.12.012. eCollection 2014. Neuroimage Clin. 2014. PMID: 24634832 Free PMC article.
-
Predicting Conversion from Subjective Cognitive Decline to Mild Cognitive Impairment and Alzheimer's Disease Dementia Using Ensemble Machine Learning.J Alzheimers Dis. 2023;93(1):125-140. doi: 10.3233/JAD-221002. J Alzheimers Dis. 2023. PMID: 36938735
-
Combination of Plasma Neurofilament Light Chain and Mini-Mental State Examination Score Predicts Progression from Mild Cognitive Impairment to Alzheimer's Disease within 5 Years.J Alzheimers Dis. 2021;82(3):951-964. doi: 10.3233/JAD-210092. J Alzheimers Dis. 2021. PMID: 34120902
-
Prediction Models for Conversion From Mild Cognitive Impairment to Alzheimer's Disease: A Systematic Review and Meta-Analysis.Front Aging Neurosci. 2022 Apr 7;14:840386. doi: 10.3389/fnagi.2022.840386. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35493941 Free PMC article.
-
Digital Clock and Recall is superior to the Mini-Mental State Examination for the detection of mild cognitive impairment and mild dementia.Alzheimers Res Ther. 2024 Jan 2;16(1):2. doi: 10.1186/s13195-023-01367-7. Alzheimers Res Ther. 2024. PMID: 38167251 Free PMC article. Review.
Cited by
-
Cell-Free DNA As Peripheral Biomarker of Alzheimer's Disease.Aging Dis. 2024 Mar 29;16(2):787-803. doi: 10.14336/AD.2024.0329. Aging Dis. 2024. PMID: 38607732 Free PMC article. Review.
-
Cancer Immunotherapy Based on the Bidirectional Reprogramming of the Tumor Microenvironment by a "Brakes Off/ Step on the Accelerator" Core-Shell Manganese Phosphate/siPD-L1 Modulator.Exploration (Beijing). 2025 Feb 9;5(3):270009. doi: 10.1002/EXP.70009. eCollection 2025 Jun. Exploration (Beijing). 2025. PMID: 40585771 Free PMC article.
-
Development of an automated artificial intelligence-based system for urogenital schistosomiasis diagnosis using digital image analysis techniques and a robotized microscope.PLoS Negl Trop Dis. 2024 Nov 5;18(11):e0012614. doi: 10.1371/journal.pntd.0012614. eCollection 2024 Nov. PLoS Negl Trop Dis. 2024. PMID: 39499735 Free PMC article.
-
Mechanistic modelling of allergen-induced airways disease in early life.Sci Rep. 2025 Jan 2;15(1):368. doi: 10.1038/s41598-024-83204-x. Sci Rep. 2025. PMID: 39747954 Free PMC article.
-
Limited generalizability and high risk of bias in multivariable models predicting conversion risk from mild cognitive impairment to dementia: A systematic review.Alzheimers Dement. 2025 Apr;21(4):e70069. doi: 10.1002/alz.70069. Alzheimers Dement. 2025. PMID: 40189799 Free PMC article.
References
-
- Livingston G., Huntley J., Sommerlad A., Ames D., Ballard C., Banerjee S., Brayne C., Burns A., Cohen-Mansfield J., Cooper C., et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet Lond. Engl. 2020;396:413–446. doi: 10.1016/S0140-6736(20)30367-6. - DOI - PMC - PubMed
-
- Alzheimer’s Association 2022 Alzheimer’s Disease Facts & Figures Special Report. Alzheimers Dement 2022; 18. 2022-Facts-and-Figures-Report_1.pdf () [(accessed on 23 July 2023)]. Available online: http://www.alz.org.
Grants and funding
LinkOut - more resources
Full Text Sources
