

Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis
- PMID: 38201423
- PMCID: PMC10795679
- DOI: 10.3390/diagnostics14010113
Diagnostic Accuracy of MRI in Detecting the Perineural Spread of Head and Neck Tumors: A Systematic Review and Meta-Analysis
Abstract
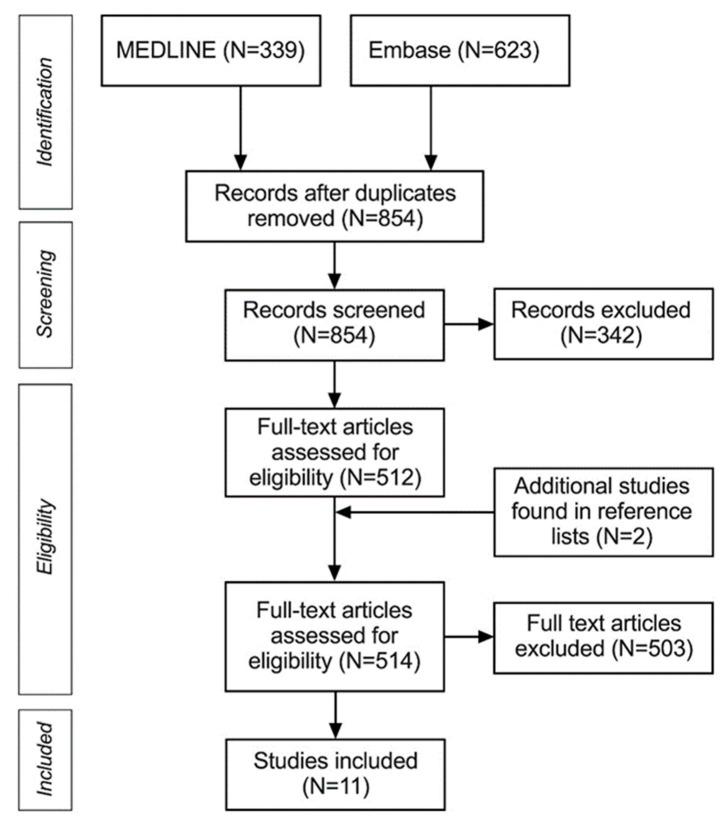
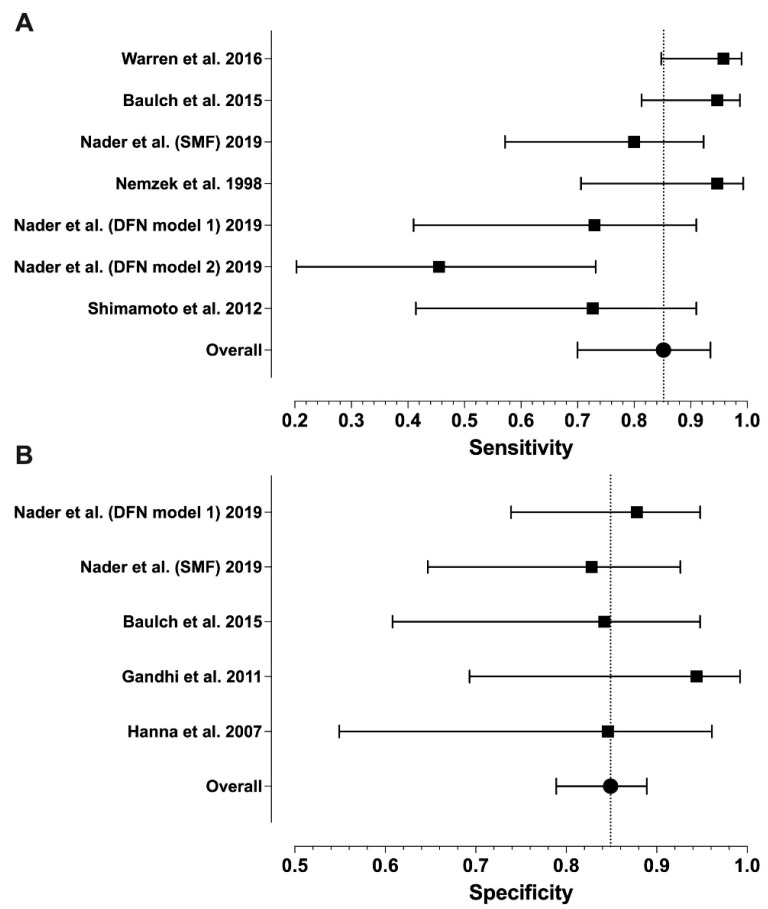
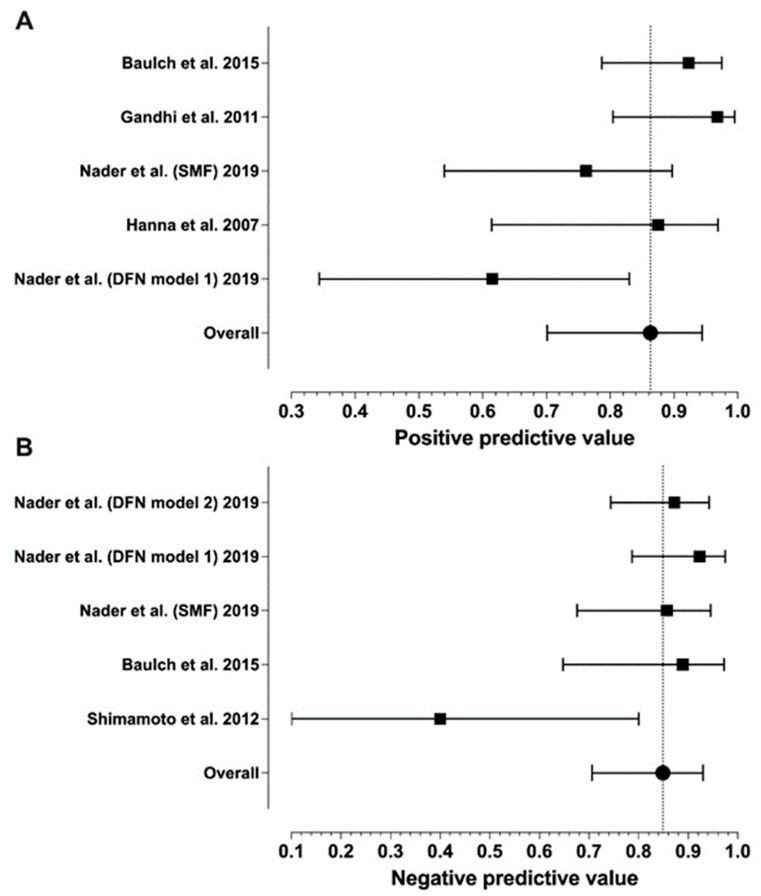
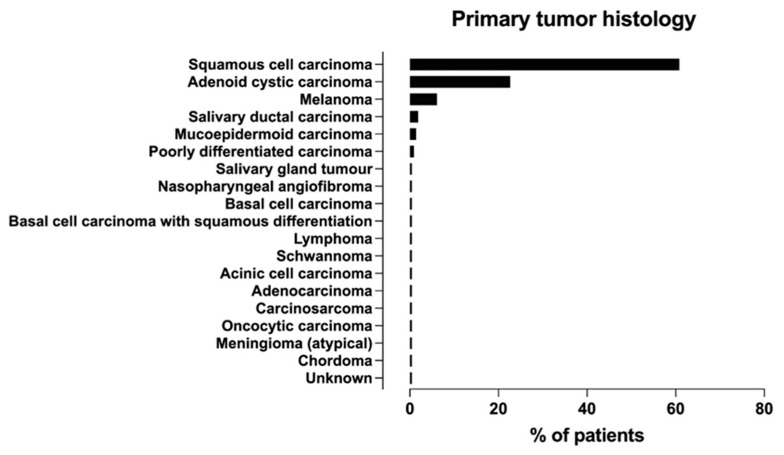
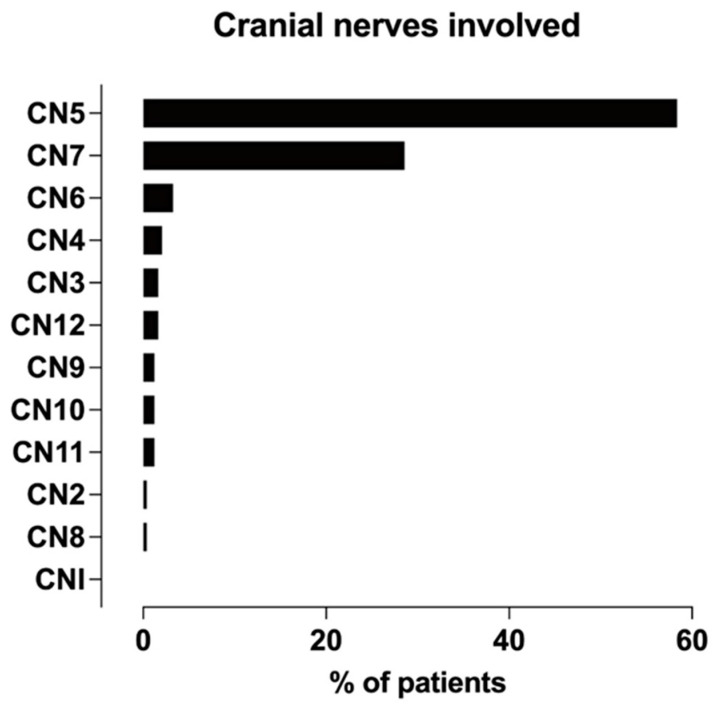
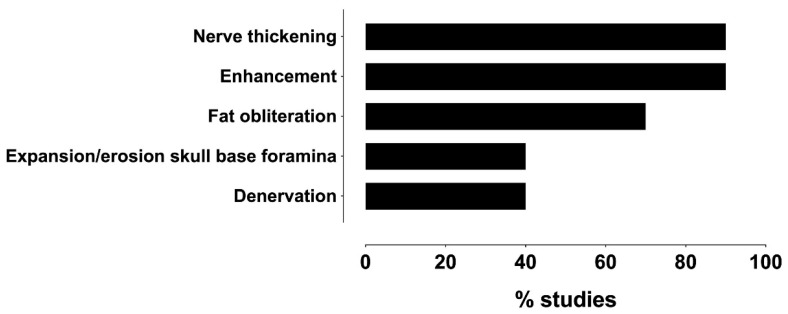
The purpose of this study was to review the diagnostic accuracy of MRI in detecting perineural spreading (PNS) of head and neck tumors using histopathological or surgical evidence from the afflicted nerve as the reference standard. Previous studies in the English language published in the last 30 years were searched from PubMed and Embase databases. We included studies that used magnetic resonance imaging (MRI) (with and without contrast enhancement) to detect PNS, as well as the histological or surgical confirmation of PNS, and that reported the exact numbers of patients required for assessing diagnostic accuracy. The outcome measures were sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Heterogeneity was assessed with the Higgins inconsistency test (I2). P-values smaller than 0.05 were considered statistically significant. A total of 11 retrospective studies were found, reporting 319 nerve samples from 245 patients. Meta-analytic estimates and their 95% confidence intervals were as follows: sensitivity 0.85 (0.70-0.95), specificity 0.85 (0.80-0.89), PPV 0.86 (0.70-0.94), and NPV 0.85 (0.71-0.93). We found statistically significant heterogeneity for sensitivity (I2 = 72%, p = 0.003) and PPV (I2 = 70%, p = 0.038), but not for NPV (I2 = 65%, p = 0.119) or specificity (I2 = 12%, p = 0.842). The most frequent MRI features of PNS were nerve enlargement and enhancement. Squamous cell carcinoma and adenoid cystic carcinoma were the most common tumor types, and the facial and trigeminal nerves were the most commonly affected nerves in PNS. Only a few studies provided examples of false MRI diagnoses. MRI demonstrated high diagnostic accuracy in depicting PNS of cranial nerves, yet this statement was based on scarce and heterogeneous evidence.
Keywords: cranial nerves; head and neck tumors; magnetic resonance imaging; meta-analysis; perineural spread; systematic review.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
Similar articles
-
The sensitivity and specificity of high-resolution imaging in evaluating perineural spread of adenoid cystic carcinoma to the skull base.Arch Otolaryngol Head Neck Surg. 2007 Jun;133(6):541-5. doi: 10.1001/archotol.133.6.541. Arch Otolaryngol Head Neck Surg. 2007. PMID: 17576903
-
Diagnostic Accuracy of MRI for Orbital and Intracranial Invasion of Sinonasal Malignancies: A Systematic Review and Meta-Analysis.J Clin Med. 2024 Dec 12;13(24):7556. doi: 10.3390/jcm13247556. J Clin Med. 2024. PMID: 39768479 Free PMC article. Review.
-
Diagnostic Accuracy of Contrast-Enhanced MRI for Detection of Perineural Spread in Head and Neck Cancer: A Systematic Review and Meta-Analysis.J Neurol Surg B Skull Base. 2023 Dec 22;85(Suppl 2):e97-e109. doi: 10.1055/s-0043-1777793. eCollection 2024 Oct. J Neurol Surg B Skull Base. 2023. PMID: 39444772 Free PMC article.
-
Does PET scan have any role in the diagnosis of perineural spread associated with the head and neck tumors?Adv Clin Exp Med. 2022 Aug;31(8):827-835. doi: 10.17219/acem/147359. Adv Clin Exp Med. 2022. PMID: 35467086
-
Perineural Spread of Tumor in the Skull Base and Head and Neck.Oral Maxillofac Surg Clin North Am. 2023 Aug;35(3):399-412. doi: 10.1016/j.coms.2023.02.004. Epub 2023 Mar 31. Oral Maxillofac Surg Clin North Am. 2023. PMID: 37005170 Review.
Cited by
-
Development of a clinical diagnostic model for Bell's palsy in patients with facial muscle weakness.Biomol Biomed. 2024 Oct 17;24(6):1795-1805. doi: 10.17305/bb.2024.10677. Biomol Biomed. 2024. PMID: 38920750 Free PMC article.
-
Molecular mechanisms and clinical significance of perineural invasion in malignancies: the pivotal role of tumor-associated Schwann cells in cancer progression and metastasis.Med Oncol. 2025 Apr 22;42(5):171. doi: 10.1007/s12032-025-02729-x. Med Oncol. 2025. PMID: 40259163 Review.
-
Assessment of peri-neural invasion in oral cancer patients using MRI: A clinical and radiologic correlation study.Bioinformation. 2025 May 31;21(5):1118-1122. doi: 10.6026/973206300211118. eCollection 2025. Bioinformation. 2025. PMID: 40822764 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
