

Congenital Tumors-Magnetic Resonance Imaging Findings with Focus on Rare Tumors
- PMID: 38201471
- PMCID: PMC10778132
- DOI: 10.3390/cancers16010043
Congenital Tumors-Magnetic Resonance Imaging Findings with Focus on Rare Tumors
Abstract
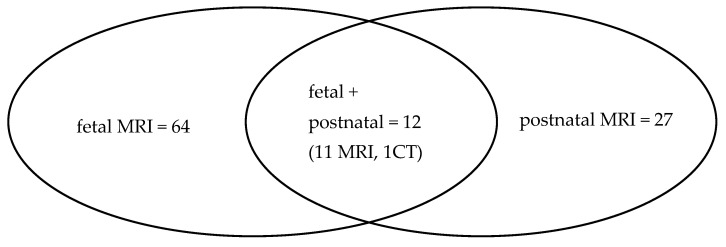
Congenital tumors are rare and, owing to this rarity, there is limited information on many of them. A total of 839 fetal and postnatal MRI studies performed in the first 3 months of life were retrospectively reviewed. They were performed with the use of 1.5 T scanners. Seventy-six tumors were diagnosed based on fetal MRI between 20 and 37 gestational weeks, and 27 were found after birth, from 1 day of age to 3 months of life. Teratomas were the most common tumors in our dataset, mainly in the sacrococcygeal region (SCT), followed by cardiac rhabdomyomas and subependymal giant cell astrocytomas (SEGA) associated with TSC, and neuroblastomas. The group of less common tumors consisted of infantile fibrosarcomas, malignant rhabdoid tumors, mesoblastic nephromas and Wilms tumor, craniopharyngiomas, brain stem gliomas, desmoplastic infantile astrocytoma, choroid plexus carcinoma, glioblastoma, hemangiopericytoma, rhabdomyosarcoma, melanoma, mesenchymal hamartomas of the chest wall and the liver, and juvenile xanthogranuloma, with special consideration of blue rubber bleb nevus syndrome. MRI plays a significant role in further and better characterization of congenital tumors, leading to a correct diagnosis in many cases, which is crucial for pregnancy and neonatal management and psychological preparation of the parents. No diagnosis is impossible and can be absolutely excluded.
Keywords: congenital tumor; fetus; infant; magnetic resonance imaging (MRI).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures













References
LinkOut - more resources
Full Text Sources
