

Stereotactic Radiosurgery for Women Older than 65 with Breast Cancer Brain Metastases
- PMID: 38201564
- PMCID: PMC10778270
- DOI: 10.3390/cancers16010137
Stereotactic Radiosurgery for Women Older than 65 with Breast Cancer Brain Metastases
Abstract
Background: Breast cancer is the second most common cause of brain metastases (BM). Despite increasing incidence of BM in older women, there are limited data on the optimal management of BM in this age group. In this study, we assessed the survival outcomes and treatment patterns of older breast cancer patients ≥65 years old with BM compared to younger patients at our institution.
Methods: An IRB-approved single-institutional retrospective review of biopsy-proven breast cancer patients with BM treated with 1- to 5-fraction stereotactic radiation therapy (SRS) from 2015 to 2020 was performed. Primary endpoint was intracranial progression-free survival (PFS) defined as the time interval between the end of SRS to the date of the first CNS progression. Secondary endpoints were overall survival (OS) from the end of SRS and radiation treatment patterns. Kaplan-Meier estimates and Cox proportional hazard regression method were used for survival analyses.
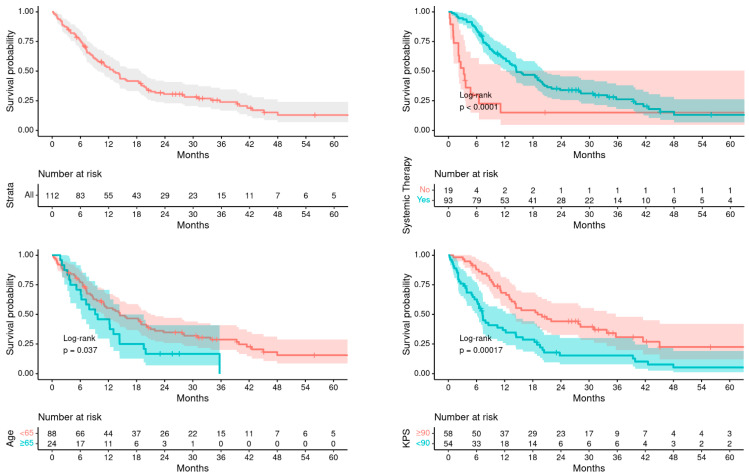
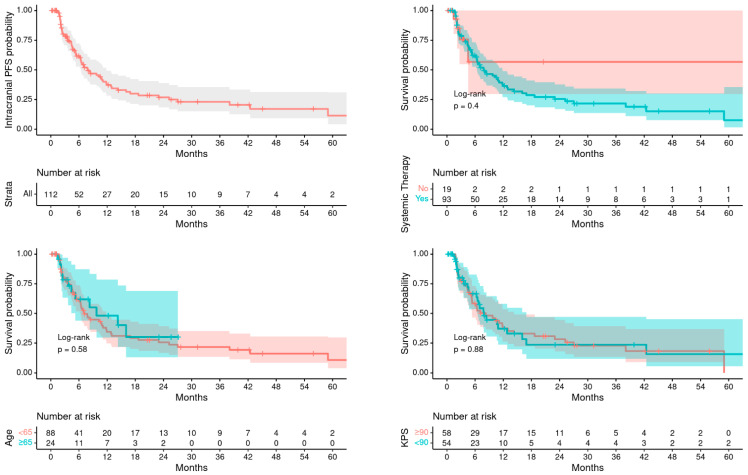
Results: A total of 112 metastatic breast cancer patients with BMs were included of which 24 were ≥65 years old and 88 were <65 years old. Median age at RT was 72 years (range 65-84) compared to 52 years (31-64) in younger patients. There were significantly higher number of older women with ER/PR positive disease (75% vs. 49%, p = 0.036), while younger patients were more frequently triple negative (32% vs. 12%, p = 0.074) and HER2 positive (42% vs. 29%, p = 0.3). Treatment-related adverse events were similar in both groups. Overall, 14.3% patients had any grade radiation necrosis (RN) (older vs. young: 8.3% vs. 16%, p = 0.5) while 5.4% had grade 3 or higher RN (0% vs. 6.8%, p = 0.7). Median OS after RT was poorer in older patients compared to younger patients (9.5 months vs. 14.5 months, p = 0.037), while intracranial PFS from RT was similar between the two groups (9.7 months vs. 7.1 months, p = 0.580). On univariate analysis, significant predictors of OS were age ≥65 years old (hazard risk, HR = 1.70, p = 0.048), KPS ≤ 80 (HR = 2.24, p < 0.001), HER2 positive disease (HR = 0.46, p < 0.001), isolated CNS metastatic disease (HR = 0.29, p < 0.001), number of brain metastases treated with RT (HR = 1.06, p = 0.028), and fractionated SRS (HR = 0.53, p = 0.013). On multivariable analysis, KPS ≤ 80, HER2 negativity and higher number of brain metastases predicted for poorer survival, while age was not a significant factor for OS after adjusting for other variables. Patients who received systemic therapy after SRS had a significantly improved OS on univariate and multivariable analysis (HR = 0.32, p < 0.001). Number of brain metastases treated was the only factor predictive of worse PFS (HR = 1.06, p = 0.041), which implies a 6% additive risk of progression for every additional metastasis treated.
Conclusions: Although older women had poorer OS than younger women, OS was similar after adjusting for KPS, extracranial progression, and systemic therapy; and there was no difference in rates of intracranial PFS, neurological deaths, and LMD in the different age groups. This study suggests that age alone may not play an independent role in treatment-selection and that outcomes for breast cancer patients with BMs and personalized decision-making including other clinical factors should be considered. Future studies are warranted to assess neurocognitive outcomes and other radiation treatment toxicities in older patients.
Keywords: breast cancer; geriatric cancer; oligometastases; radiation therapy; stereotactic radiosurgery.
Conflict of interest statement
The authors declare no relevant conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
