

Location Has Prognostic Impact on the Outcome of Colorectal Mucinous Adenocarcinomas
- PMID: 38201574
- PMCID: PMC10778219
- DOI: 10.3390/cancers16010147
Location Has Prognostic Impact on the Outcome of Colorectal Mucinous Adenocarcinomas
Abstract
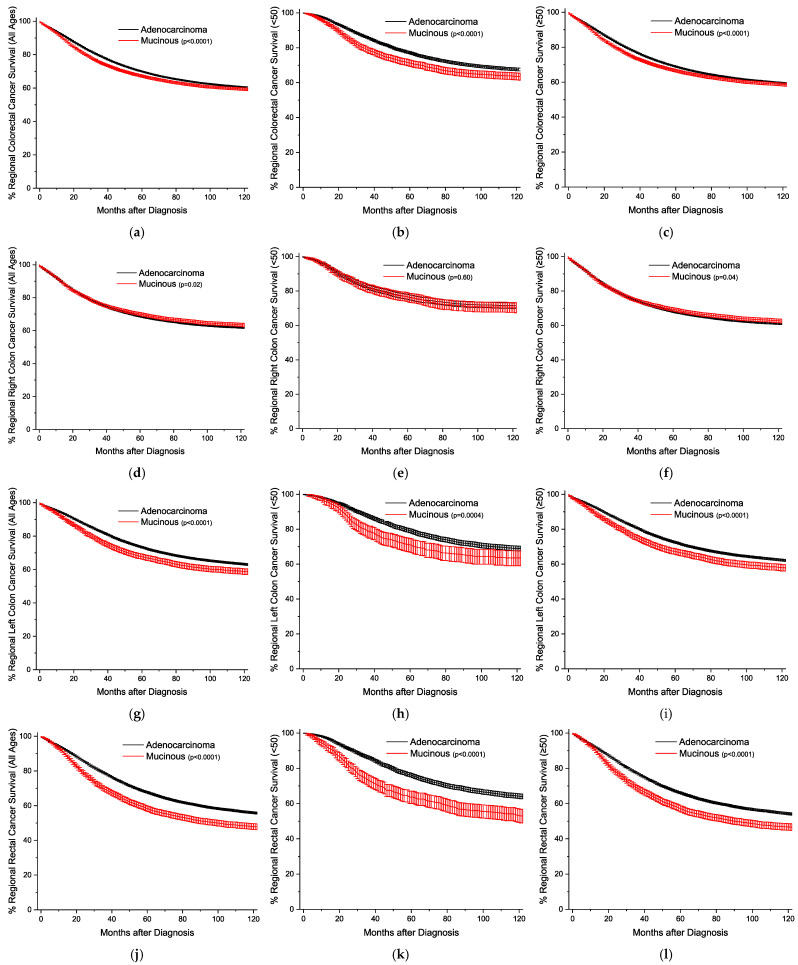
Mucinous (colloid) adenocarcinomas (MAs) are a rare histological subtype of tumors defined by extracellular mucin comprising more than 50% of the tumor. These tumors are on a continuum of mucin-producing malignancies with signet ring cell adenocarcinomas (SRCCs), which instead produce intracellular mucin. Mucin-containing cancers occur primarily in the stomach and colon, where for SRCCs, outcomes are relatively worse in the proximal stomach and the rectum. It is not known if MAs have similar outcomes. In this study, we use the Surveillance, Epidemiology, and End Results (SEER) database to examine the effects of tumor localization, age, sex, and stage on colorectal and gastric cancer outcomes for MAs. For right colon cancers, MAs are more common, particularly in females, and have slightly better or equivalent outcomes across all stages and ages compared to conventional adenocarcinomas, but outcomes are progressively worse compared to conventional adenocarcinomas for left colon and rectal cancers. Unlike SRCCs, MAs have similar outcomes to conventional adenocarcinomas in all stomach locations. Overall, these results suggest that MAs have an intrinsically different tumor biology in the left colon and rectum that promotes pathogenesis. Decoding this phenomenon could lead to more effectively tailored patient treatment regimens.
Keywords: cancer; chemotherapy; colloid adenocarcinomas; epidemiology; histopathology; radiotherapy; signet ring cell adenocarcinomas; surgery; survival outcomes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Digestive System Tumours, Who Classification of tumours Series. 5th ed. International Agency for Research on Cancer; Lyon, France: 2019.
Grants and funding
LinkOut - more resources
Full Text Sources
