

New Frontiers in Monoclonal Antibodies for Relapsed/Refractory Diffuse Large B-Cell Lymphoma
- PMID: 38201614
- PMCID: PMC10778309
- DOI: 10.3390/cancers16010187
New Frontiers in Monoclonal Antibodies for Relapsed/Refractory Diffuse Large B-Cell Lymphoma
Abstract
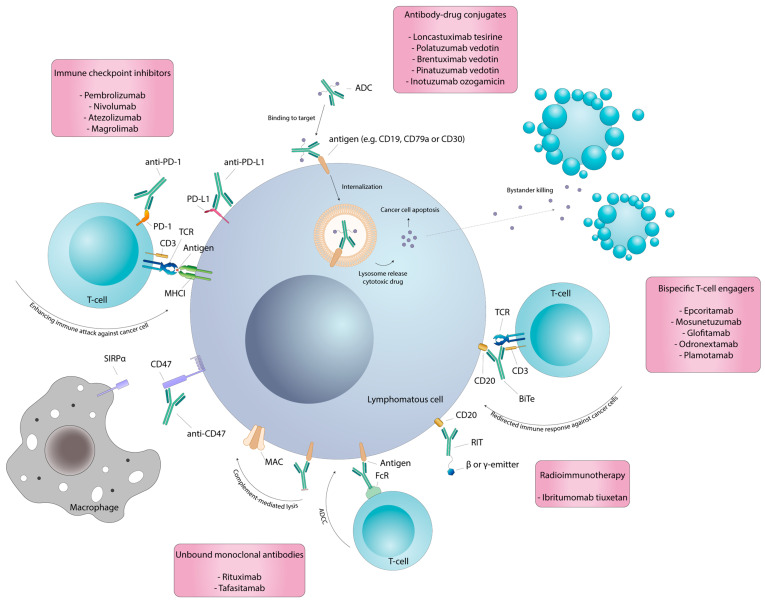
Diffuse large B-cell lymphoma (DLBCL) is the most common aggressive lymphoma. Approximately 60% of patients are cured with R-CHOP as a frontline treatment, while the remaining patients experience primary refractory or relapsed disease (R/R). The prognosis for R/R DLBCL patients who are neither eligible for autologous stem-cell transplantations nor CAR-T-cell treatment is poor, representing an important unmet need. Monoclonal antibodies (mAbs) have dramatically improved therapeutic options in anti-cancer strategies, offering new opportunities to overcome chemo-refractoriness in this challenging disease, even in cases of primary non-responder DLBCL. Several novel mAbs, characterized by different mechanisms of action and targets, are now available for R/R DLBCL. Unbound mAbs induce an immune response against cancer cells, triggering different mechanisms, including antibody-dependent cellular cytotoxicity (ADCC), activation of antibody-dependent cell-mediated phagocytosis (ADCP) and complement-dependent cytotoxicity (CDC). Antibody-drug conjugates (ADCs) and radioimmunotherapy (RIT), respectively, deliver a cytotoxic payload or a beta-emitter radionuclide to the targeted cells and nearby bystanders. Bispecific T-cell engagers (BiTes) and immune checkpoint inhibitors (ICIs) redirect and enhance the immune response against tumor cells. Here, we review therapeutic strategies based on monoclonal antibodies for R/R DLBCL.
Keywords: antibody-dependent cellular cytotoxicity; bispecific antibodies; diffuse large B-cell lymphoma; immune checkpoint inhibitors; monoclonal antibodies; target therapy.
Conflict of interest statement
M.S., R.B., G.M.-C., A.M.M., W.A.E. and G.M.R. have nothing to declare. G.G. declares advisory board and speaker’s bureau honoraria from AbbVie, AstraZeneca, BeiGene, Hikma, Incyte, Janssen and Lilly.
Figures
References
-
- Perry A.M., Diebold J., Nathwani B.N., Maclennan K.A., Müller-Hermelink H.K., Bast M., Boilesen E., Armitage J.O., Weisenburger D.D. Non-Hodgkin Lymphoma in the Developing World: Review of 4539 Cases from the International Non-Hodgkin Lymphoma Classification Project. Haematologica. 2016;101:1244–1250. doi: 10.3324/haematol.2016.148809. - DOI - PMC - PubMed
-
- Smith A., Crouch S., Lax S., Li J., Painter D., Howell D., Patmore R., Jack A., Roman E. Lymphoma Incidence, Survival and Prevalence 2004–2014: Sub-Type Analyses from the UK’s Haematological Malignancy Research Network. Br. J. Cancer. 2015;112:1575–1584. doi: 10.1038/bjc.2015.94. - DOI - PMC - PubMed
-
- Coiffier B., Lepage E., Brière J., Herbrecht R., Tilly H., Bouabdallah R., Morel P., Van Den Neste E., Salles G., Gaulard P., et al. Chop Chemotherapy plus Rituximab Compared with Chop Alone in Elderly Patients with Diffuse Large-B-Cell Lymphoma. N. Engl. J. Med. 2002;346:235–242. doi: 10.1056/NEJMoa011795. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
