

Prediction of 177Lu-DOTATATE Therapy Outcomes in Neuroendocrine Tumor Patients Using Semi-Automatic Tumor Delineation on 68Ga-DOTATATE PET/CT
- PMID: 38201627
- PMCID: PMC10778298
- DOI: 10.3390/cancers16010200
Prediction of 177Lu-DOTATATE Therapy Outcomes in Neuroendocrine Tumor Patients Using Semi-Automatic Tumor Delineation on 68Ga-DOTATATE PET/CT
Abstract
Background: Treatment of metastatic neuroendocrine tumors (NET) with 177Lu-DOTATATE peptide receptor radionuclide therapy (PRRT) results in favorable response only in a subset of patients. We investigated the prognostic value of quantitative pre-treatment semi-automatic 68Ga-DOTATATE PET/CT analysis in NET patients treated with PRRT.
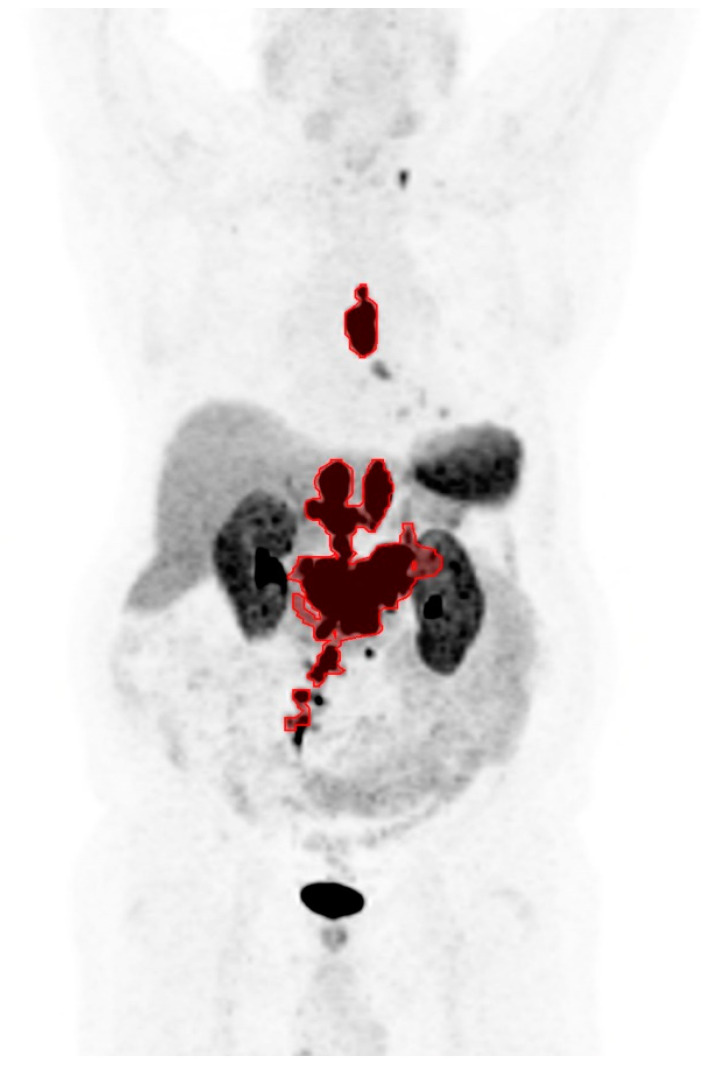
Methods: The medical records of 94 NET patients who received at least one cycle of PRRT at a single institution were retrospectively reviewed. On each pre-treatment 68Ga-DOTATATE PET/CT, the total tumor volume (TTV), maximum tumor standardized uptake value for the patient (SUVmax), and average uptake in the lesion with the lowest radiotracer uptake (SUVmin) were determined with a semi-automatic tumor delineation method. Progression-free survival (PFS) and overall survival (OS) among the patients were compared based on optimal cutoff values for the imaging parameters.
Results: On Kaplan-Meier analysis and univariate Cox regression, significantly shorter PFS was observed in patients with lower SUVmax, lower SUVmin, and higher TTV. On multivariate Cox regression, lower SUVmin and higher TTV remained predictive of shorter PFS. Only higher TTV was found to be predictive of shorter OS on Kaplan-Meier and Cox regression analyses. In a post hoc Kaplan-Meier analysis, patients with at least one high-risk feature (low SUVmin or high TTV) showed shorter PFS and OS, which may be the most convenient parameter to measure in clinical practice.
Conclusions: The tumor volume and lowest lesion uptake on 68Ga-DOTATATE PET/CT can predict disease progression following PRRT in NET patients, with the former also predictive of overall survival. NET patients at risk for poor outcomes following PRRT can be identified with semi-automated quantitative analysis of 68Ga-DOTATATE PET/CT.
Keywords: 177Lu-DOTATATE; 68Ga-DOTATATE; neuroendocrine tumor; positron emission tomography computed tomography; prognostic factor.
Conflict of interest statement
R.N. is an employee of MIM Software Inc. J.R.E. discloses employment-spouse at Janssen, advisory board/consultant at Merck, and institutional research support from Seagen, Merck, Gilead, Oncolys, Hutchmed, Arcus, Amgen, and Replimune. D.A.P. discloses research funding from Lantheus, Point Biopharma, and Fusion Pharmaceuticals; honoraria from Molecular Targeting Technologies Inc.; and stock options from Molecular Targeting Technologies Inc. and Trevarx. The other authors declare no conflict of interest relevant to the study.
Figures




Similar articles
-
Prevalence of hitherto unknown brain meningioma detected on 68Ga-DOTATATE positron-emission tomography/computed tomography in patients with metastatic neuroendocrine tumor and exploring potential of 177Lu-DOTATATE peptide receptor radionuclide therapy as single-shot treatment approach targeting both tumors.World J Nucl Med. 2019 Apr-Jun;18(2):160-170. doi: 10.4103/wjnm.WJNM_39_18. World J Nucl Med. 2019. PMID: 31040748 Free PMC article.
-
Visual and whole-body quantitative analyses of 68 Ga-DOTATATE PET/CT for prognosis of outcome after PRRT with 177Lu-DOTATATE.Ann Nucl Med. 2024 Apr;38(4):296-304. doi: 10.1007/s12149-023-01899-w. Epub 2024 Jan 22. Ann Nucl Med. 2024. PMID: 38252228
-
Clinical utility of 177 Lu-DOTATATE PRRT in somatostatin receptor-positive metastatic medullary carcinoma of thyroid patients with assessment of efficacy, survival analysis, prognostic variables, and toxicity.Head Neck. 2020 Mar;42(3):401-416. doi: 10.1002/hed.26024. Epub 2019 Nov 22. Head Neck. 2020. PMID: 31755622
-
Semi-automated segmentation methods of SSTR PET for dosimetry prediction in refractory meningioma patients treated by SSTR-targeted peptide receptor radionuclide therapy.Eur Radiol. 2023 Oct;33(10):7089-7098. doi: 10.1007/s00330-023-09697-8. Epub 2023 May 6. Eur Radiol. 2023. PMID: 37148355 Review.
-
Gastroenteropancreatic Neuroendocrine Tumor Diagnosis: DOTATATE PET/CT.PET Clin. 2023 Apr;18(2):189-200. doi: 10.1016/j.cpet.2022.11.001. Epub 2022 Dec 28. PET Clin. 2023. PMID: 36585339 Review.
Cited by
-
Epigenetic dysregulation in cancer: mechanisms, diagnostic biomarkers and therapeutic strategies.Med Oncol. 2025 Jul 21;42(8):359. doi: 10.1007/s12032-025-02905-z. Med Oncol. 2025. PMID: 40691387 Review.
-
Retrospective evaluation of the predictive value of tumour burden at baseline [68 Ga]Ga-DOTA-TOC or -TATE PET/CT and tumour dosimetry in GEP-NET patients treated with PRRT.EJNMMI Rep. 2024 Aug 8;8(1):24. doi: 10.1186/s41824-024-00210-y. EJNMMI Rep. 2024. PMID: 39112915 Free PMC article.
-
Hemophagocytic lymphohistiocytosis: current treatment advances, emerging targeted therapy and underlying mechanisms.J Hematol Oncol. 2024 Nov 7;17(1):106. doi: 10.1186/s13045-024-01621-x. J Hematol Oncol. 2024. PMID: 39511607 Free PMC article. Review.
-
Prognostic significance of systemic immune-inflammation index in hepatocellular carcinoma: a meta-analysis.Clin Transl Oncol. 2025 Aug 19. doi: 10.1007/s12094-025-04028-3. Online ahead of print. Clin Transl Oncol. 2025. PMID: 40828354 Review.
-
Synthesis, anticancer activity, and molecular docking of half-sandwich iron(II) cyclopentadienyl complexes with maleimide and phosphine or phosphite ligands.Sci Rep. 2024 Mar 7;14(1):5634. doi: 10.1038/s41598-024-56339-0. Sci Rep. 2024. PMID: 38454122 Free PMC article.
References
-
- Yao J.C., Hassan M., Phan A., Dagohoy C., Leary C., Mares J.E., Abdalla E.K., Fleming J.B., Vauthey J.N., Rashid A., et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008;26:3063–3072. doi: 10.1200/JCO.2007.15.4377. - DOI - PubMed
-
- Qian Z.R., Li T., Ter-Minassian M., Yang J., Chan J.A., Brais L.K., Masugi Y., Thiaglingam A., Brooks N., Nishihara R., et al. Association between Somatostatin Receptor Expression and Clinical Outcomes in Neuroendocrine Tumors. Pancreas. 2016;45:1386–1393. doi: 10.1097/MPA.0000000000000700. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
