

Concealed Inherited Cardiomyopathies Detected in Cardio-Oncology Screening
- PMID: 38202009
- PMCID: PMC10780282
- DOI: 10.3390/jcm13010002
Concealed Inherited Cardiomyopathies Detected in Cardio-Oncology Screening
Abstract
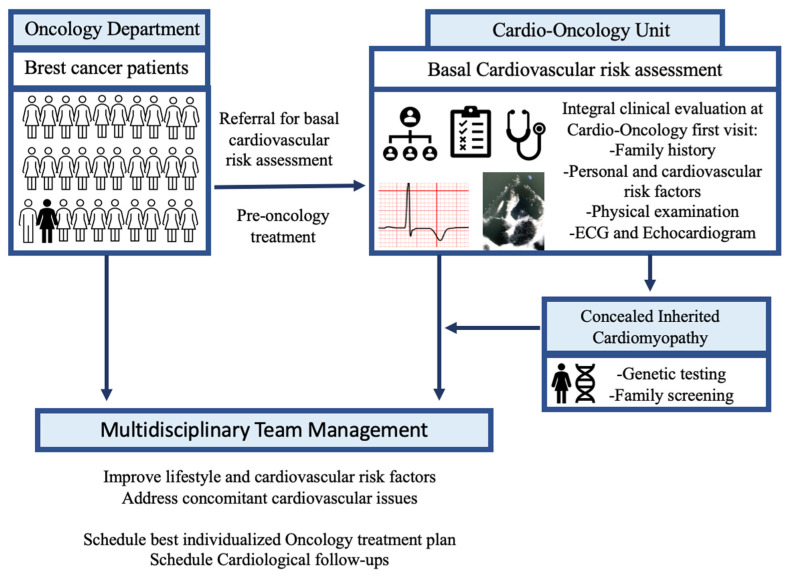
Introduction: Basal cardiovascular risk assessment in cardio-oncology is essential. Integrating clinical information, ECG and transthoracic echocardiogram can identify concealed inherited cardiomyopathies (ICMPs) with potential added risk of cardiotoxicity. We aimed to evaluate the impact of our Cardio-Oncology Unit design in detecting concealed ICMPs.
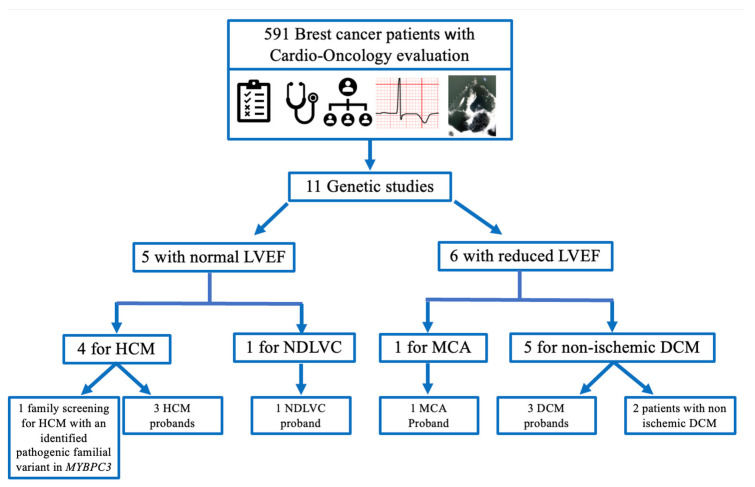
Methods: We carried out a retrospective study of all consecutive breast cancer patients referred to the Cardio-Oncology Unit for cardiac evaluation (2020-2022). ICMPs diagnosis was provided according to ESC guidelines and underwent genetic testing. ICMPs prevalence in this cohort was compared to the highest and lowest frequency reported in the general population.
Results: Among 591 breast cancer patients, we identified eight patients with ICMPs: one arrhythmogenic cardiomyopathy (ACM), three familial non-ischemic dilated cardiomyopathy (DCM), three hypertrophic cardiomyopathy (HCM) and one left ventricular non-compaction cardiomyopathy (LVNC), which has now been reclassified as non-dilated left ventricular cardiomyopathy. The number of ICMPs identified was within the expected range (neither overdiagnosed nor overlooked): ACM 0.0017 vs. 0.0002-0.001 (p 0.01-0.593); DCM 0.0051 vs. 0.002-0.0051 (p 0.094-0.676); HCM 0.005 vs. 0.0002-0.002 (p < 0.001-0.099); LVCN 0.0017 vs. 0.00014-0.013 (p 0.011-0.015). Genetic testing identified a pathogenic FLNC variant and two pathogenic TTN variants.
Conclusion: Opportunistic screening of ICMPs during basal cardiovascular risk assessment can identify high-risk cancer patients who benefit from personalized medicine and enables extension of prevention strategies to all available relatives at concealed high cardiovascular risk.
Keywords: cardio-oncology; cardiomyopathy; genetics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
"Inherited cardiovascular disease mindset" can identify concealed inherited conditions at cardio-oncology evaluation: An opportunistic screening.Int J Cardiol. 2024 Apr 15;401:131825. doi: 10.1016/j.ijcard.2024.131825. Epub 2024 Feb 1. Int J Cardiol. 2024. PMID: 38309590
-
Filamin-C variant-associated cardiomyopathy: A pooled analysis of individual patient data to evaluate the clinical profile and risk of sudden cardiac death.Heart Rhythm. 2022 Feb;19(2):235-243. doi: 10.1016/j.hrthm.2021.09.029. Epub 2021 Oct 1. Heart Rhythm. 2022. PMID: 34601126
-
The Role of Speckle Tracking Echocardiography in the Evaluation of Common Inherited Cardiomyopathies in Children and Adolescents: A Systematic Review.Diagnostics (Basel). 2021 Apr 1;11(4):635. doi: 10.3390/diagnostics11040635. Diagnostics (Basel). 2021. PMID: 33915862 Free PMC article. Review.
-
Targeted 46-gene and clinical exome sequencing for mutations causing cardiomyopathies.Mol Cell Probes. 2015 Oct;29(5):308-14. doi: 10.1016/j.mcp.2015.05.004. Epub 2015 May 12. Mol Cell Probes. 2015. PMID: 25979592
-
A Review of the Giant Protein Titin in Clinical Molecular Diagnostics of Cardiomyopathies.Front Cardiovasc Med. 2016 Jul 21;3:21. doi: 10.3389/fcvm.2016.00021. eCollection 2016. Front Cardiovasc Med. 2016. PMID: 27493940 Free PMC article. Review.
References
-
- Zamorano J.L., Lancellotti P., Rodriguez Muñoz D., Aboyans V., Asteggiano R., Galderisi M., Habib G., Lenihan D.J., Lip G.Y.H., Lyon A.R., et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC) Eur. Heart J. 2016;37:2768–2801. doi: 10.1093/eurheartj/ehw211. - DOI - PubMed
-
- Lyon A.R., López-Fernández T., Couch L.S., Asteggiano R., Aznar M.C., Bergler-Klein J., Boriani G., Cardinale D., Cordoba R., Cosyns B., et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS) Eur. Heart J. 2022;43:4229–4361. doi: 10.1093/eurheartj/ehac244. - DOI - PubMed
-
- Lancellotti P., Suter T.M., López-Fernández T., Galderisi M., Lyon A.R., Van der Meer P., Cohen Solal A., Zamorano J.-L., Jerusalem G., Moonen M., et al. Cardio-Oncology Services: Rationale, organization, and implementation. Eur. Heart J. 2019;40:1756–1763. doi: 10.1093/eurheartj/ehy453. - DOI - PubMed
-
- Lyon A.R., Dent S., Stanway S., Earl H., Brezden-Masley C., Cohen-Solal A., Tocchetti C.G., Moslehi J.J., Groarke J.D., Bergler-Klein J., et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020;22:1945–1960. - PMC - PubMed
LinkOut - more resources
Full Text Sources
