

Advancements in Basal Cell Carcinoma Diagnosis: Non-Invasive Imaging and Multimodal Approach
- PMID: 38202046
- PMCID: PMC10779576
- DOI: 10.3390/jcm13010039
Advancements in Basal Cell Carcinoma Diagnosis: Non-Invasive Imaging and Multimodal Approach
Abstract
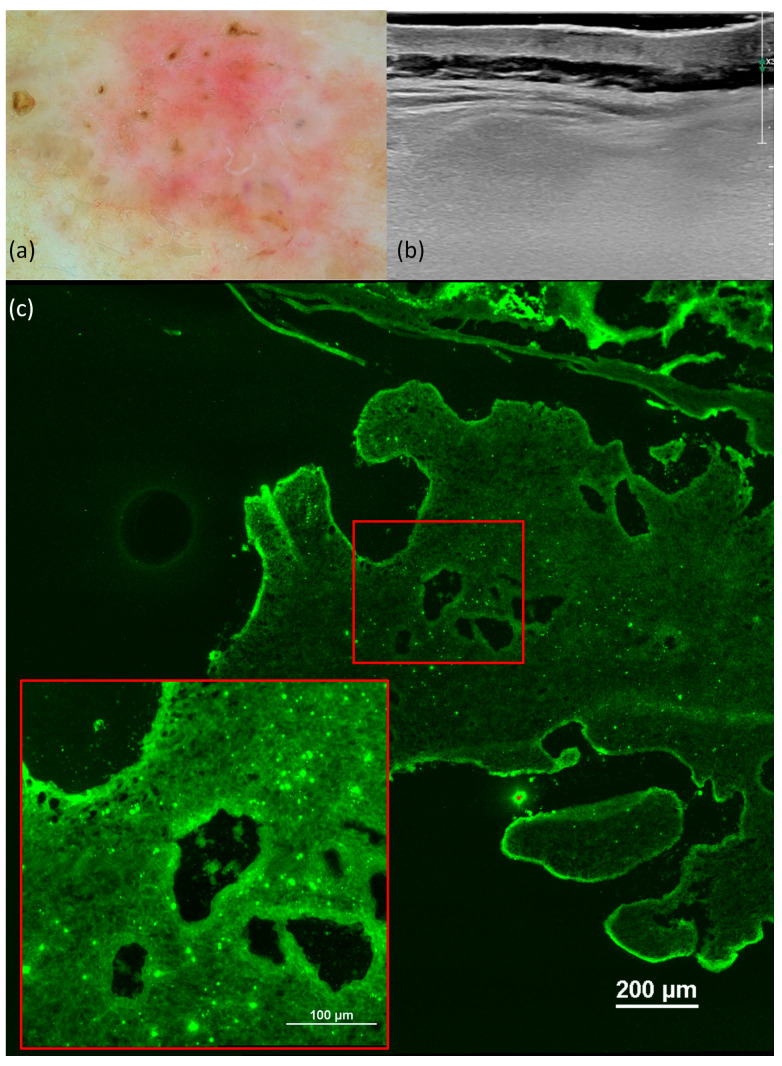
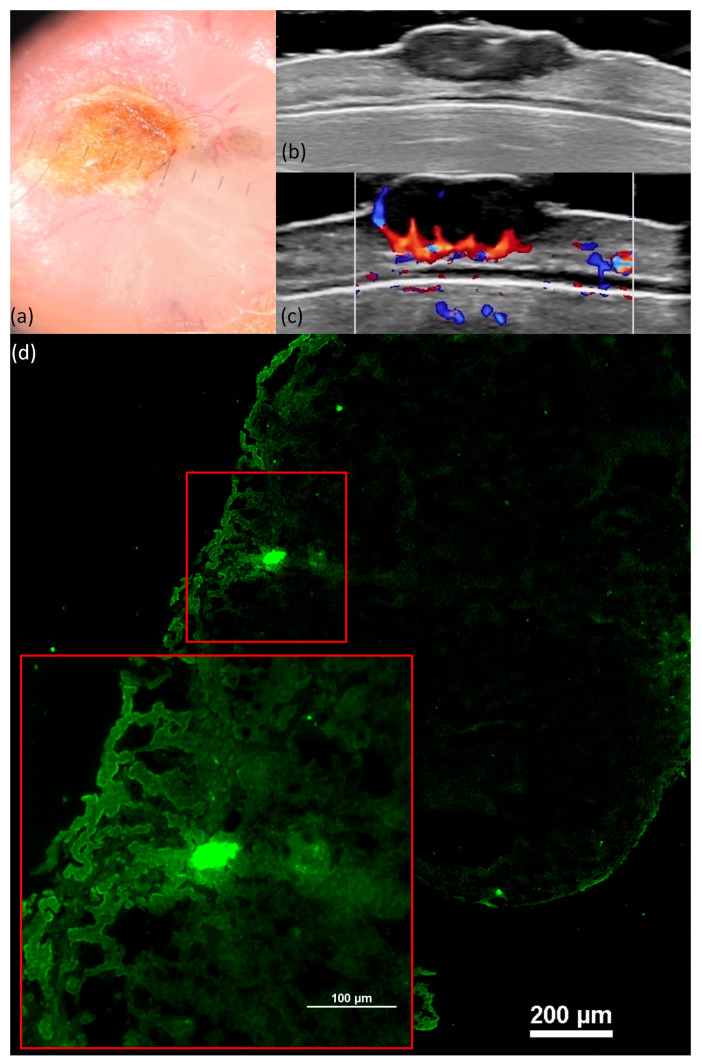
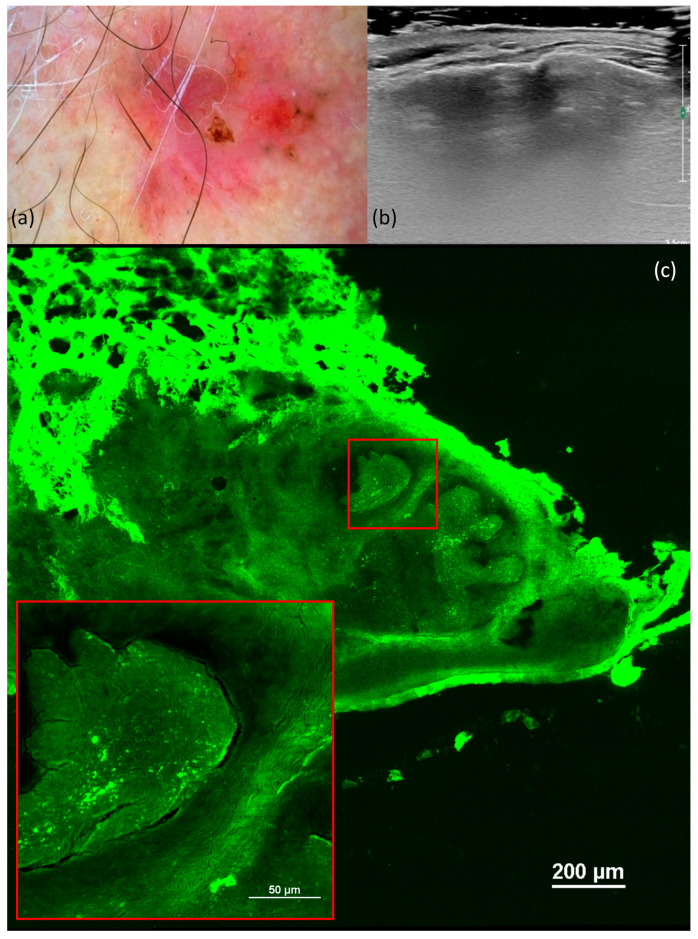
(1) Background: The aim of this study was to correlate the diagnostic criteria described in dermatoscopy, ultrasonography (US), ex vivo confocal microscopy, and histology to the most common subtypes of basal cell carcinoma (BCC). (2) Methods: We conducted a prospective study including 46 BCC cases, which were analyzed with dermatoscopy using the Delta 30 dermatoscope and Vidix 4.0 videodermoscope, with US using a high-resolution 20 MHz linear probe, with confocal microscopy, along with histopathological analysis. (3) Results: This study categorized BCC by histological subtype, with nodular being the most common (84.8%) and various other subtypes represented. US measurements of tumor thickness correlated strongly with the histopathological depth of invasion index (DI). Dermatoscopy analysis revealed significant associations between specific features and BCC subtypes. The DI was directly related to arborized vessels but inversely related to short, fine telangiectasias, maple-leaf-like areas, and spoke-wheel areas. The presence of ulceration was directly related to the DI. Confocal microscopy images exhibited several characteristics, including fluorescence, nuclear crowding, peripheral palisading, clefting, increased nuclear-cytoplasmic (N/C) ratio, and a "cauliflower-like" appearance. (4) Conclusion: The advanced detection of BCC through imagistic techniques like dermatoscopy, confocal microscopy, and ultrasound improves the diagnosis and may offer valuable insights for treatment in the future by evaluating lesion characteristics.
Keywords: basal cell carcinoma; depth of invasion index; dermatoscopy; ex vivo confocal microscopy; ultrasonography.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Classifying distinct basal cell carcinoma subtype by means of dermatoscopy and reflectance confocal microscopy.J Am Acad Dermatol. 2014 Oct;71(4):716-724.e1. doi: 10.1016/j.jaad.2014.04.067. Epub 2014 Jun 11. J Am Acad Dermatol. 2014. PMID: 24928707
-
Imaging Approach in the Diagnostics and Evaluation of the Psoriasis Plaque: A Preliminary Study and Literature Review.Diagnostics (Basel). 2024 May 7;14(10):969. doi: 10.3390/diagnostics14100969. Diagnostics (Basel). 2024. PMID: 38786267 Free PMC article.
-
Enhancing Diagnosis in Squamous Cell Carcinoma: Non-Invasive Imaging and Multimodal Approach.Diagnostics (Basel). 2025 Apr 16;15(8):1018. doi: 10.3390/diagnostics15081018. Diagnostics (Basel). 2025. PMID: 40310402 Free PMC article.
-
Dermoscopic features of basal cell carcinoma and its subtypes: A systematic review.J Am Acad Dermatol. 2021 Sep;85(3):653-664. doi: 10.1016/j.jaad.2019.11.008. Epub 2019 Nov 7. J Am Acad Dermatol. 2021. PMID: 31706938 Free PMC article.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
Cited by
-
The State of the Art of Image Guided Superficial Radiation Therapy Treatment of Non-melanoma Skin Cancer in Outpatient Dermatology Clinics in the United States and Review of the Literature.Oncol Ther. 2025 Mar;13(1):31-48. doi: 10.1007/s40487-024-00310-6. Epub 2024 Nov 21. Oncol Ther. 2025. PMID: 39572513 Free PMC article. Review.
-
Retrospective Analysis of Clinicopathological Characteristics of Surgically Treated Basal Cell Carcinomas of the Face: A Single-Centre Maxillofacial Surgery Experience.J Clin Med. 2024 Sep 14;13(18):5470. doi: 10.3390/jcm13185470. J Clin Med. 2024. PMID: 39336956 Free PMC article.
-
Dermoscopy of Basal Cell Carcinoma Part 2: Dermoscopic Findings by Lesion Subtype, Location, Age of Onset, Size and Patient Phototype.Cancers (Basel). 2025 Jan 8;17(2):176. doi: 10.3390/cancers17020176. Cancers (Basel). 2025. PMID: 39857958 Free PMC article. Review.
-
Correlation of dermoscopic and histopathological features in basal cell carcinoma using computerized image analysis.Front Med (Lausanne). 2025 Apr 30;12:1581601. doi: 10.3389/fmed.2025.1581601. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40370729 Free PMC article.
References
LinkOut - more resources
Full Text Sources
