

Myocardial Mechanics and Associated Valvular and Vascular Abnormalities in Left Ventricular Noncompaction Cardiomyopathy
- PMID: 38202085
- PMCID: PMC10779999
- DOI: 10.3390/jcm13010078
Myocardial Mechanics and Associated Valvular and Vascular Abnormalities in Left Ventricular Noncompaction Cardiomyopathy
Abstract
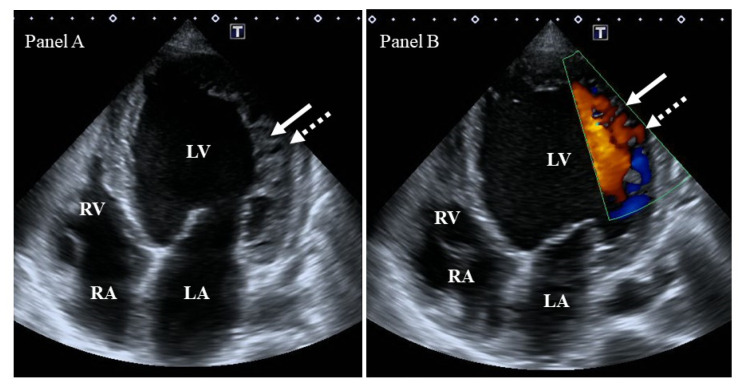
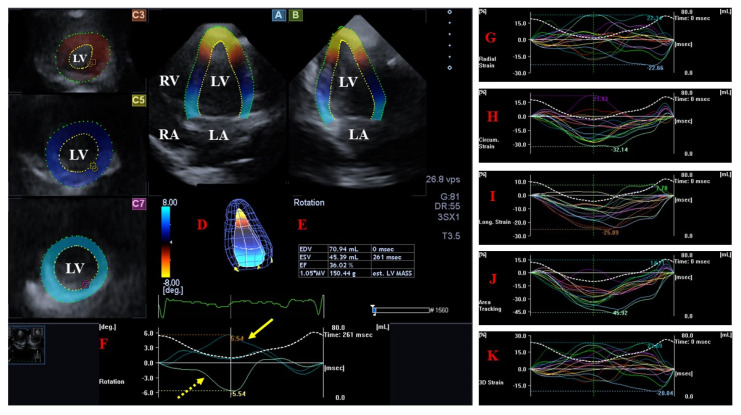
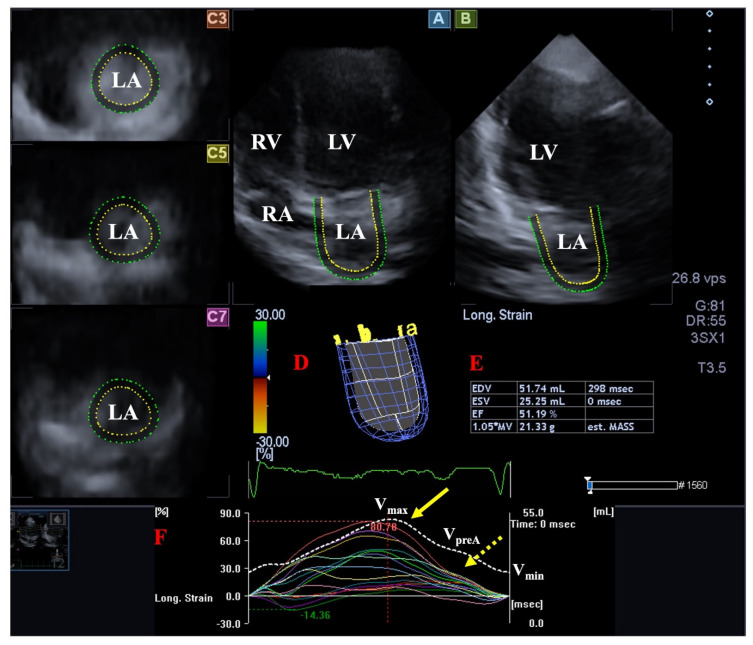
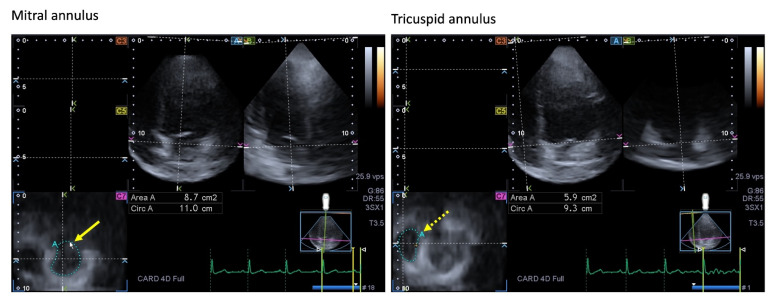
Left ventricular (LV) non-compaction (LVNC) is a rare genetic cardiomyopathy due to abnormal intra-uterine arrest of compaction of the myocardial fibers during endomyocardial embryogenesis. Due to the partial or complete absence of LV compaction, the structure of the LV wall shows characteristic abnormalities, including a thin compacted epicardium and a thick non-compacted endocardium with prominent trabeculations and deep intertrabecular recesses. LVNC is frequently associated with chronic heart failure, life-threatening ventricular arrhythmias, and systemic embolic events. According to recent findings, in the presence of LVNC, dysfunctional LV proved to be associated with left atrial volumetric and functional abnormalities and consequential dilated and functionally impaired mitral annulus, partly explaining the higher prevalence of regurgitation. Although the non-compaction process morphologically affects only the LV, signs of remodeling of the right heart were also detected. Moreover, dilation and stiffening of the aorta were present. The aim of the present detailed review was to summarize findings regarding changes in cardiac mechanics, valvular abnormalities, and vascular remodeling detected in patients with LVNC.
Keywords: cardiac mechanics; cardiomyopathy; left ventricular; non-compaction; remodeling; vascular.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
-
- Jenni R., Oechslin E., Schneider J., Attenhofer Jost C., Kaufmann P.A. Echocardiographic and pathoanatomical characteristics of isolated left ventricular noncompaction: A step towards classification as a distinct cardiomyopathy. Heart. 2001;86:666–671. doi: 10.1136/heart.86.6.666. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
