

Placenta Accreta Spectrum Prophylactic Therapy for Hyperfibrinolysis with Tranexamic Acid
- PMID: 38202142
- PMCID: PMC10780074
- DOI: 10.3390/jcm13010135
Placenta Accreta Spectrum Prophylactic Therapy for Hyperfibrinolysis with Tranexamic Acid
Abstract
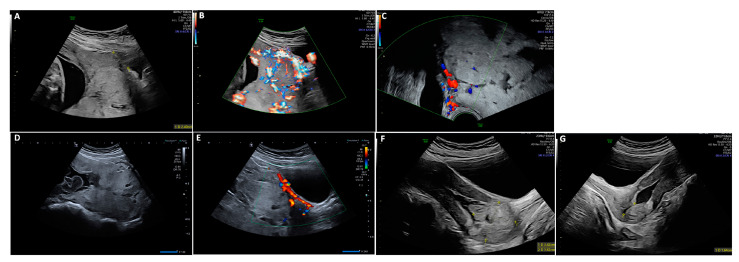
Background: To report on prophylactic therapy for hyperfibrinolysis with tranexamic acid (TXA) during expectant management (EM) in the placenta accreta spectrum (PAS).
Methods: This is a monocentric retrospective study of women with PAS presenting at our hospital between 2005 and 2021. All data were retrospectively collected through the departmental database.
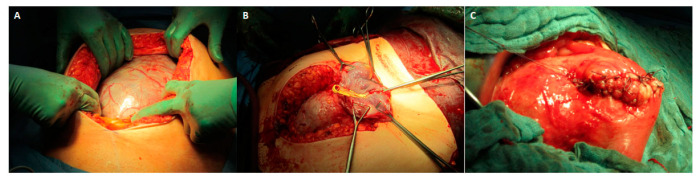
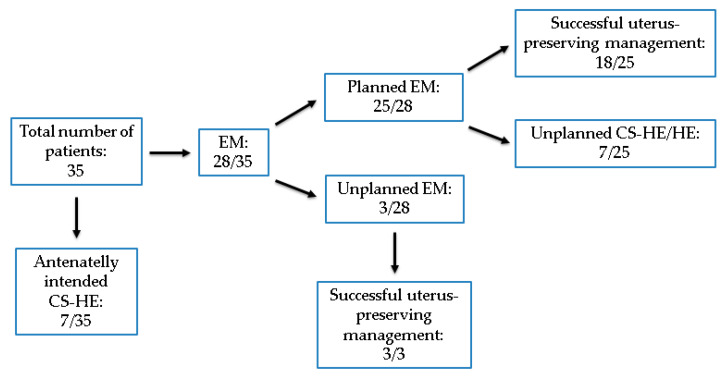
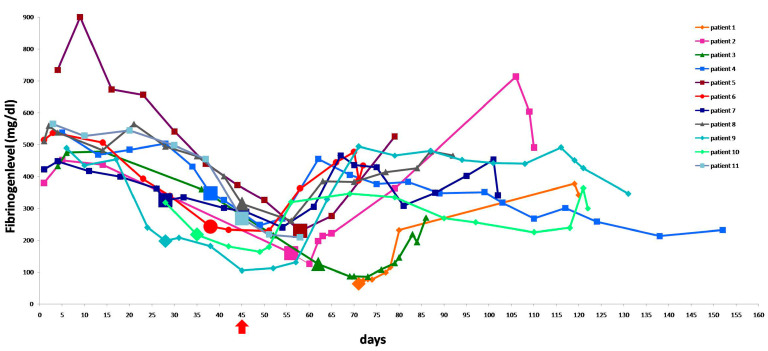
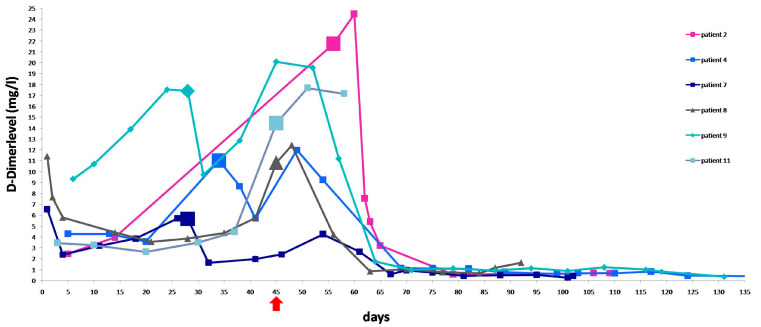
Results: 35 patients with PAS were included. EM was planned in 25 patients prior to delivery. Complete absorption of the retained placenta was seen in two patients (8%). Curettage was performed in 14 patients (56%). A hysterectomy (HE) was needed in seven (28%) patients; 18 patients (72%) underwent uterus-preserving treatment without severe complications. The mean duration of EM was 107 days. The mean day of onset of hyperfibrinolysis and beginning of TXA treatment was day 45. The mean nadir of fibrinogen level before TXA was 242.4 mg/dL, with a mean drop of 29.7% in fibrinogen level.
Conclusions: Our data support EM as a safe treatment option in PAS. Hyperfibrinolysis can be a cause of hemorrhage during EM and can be treated with TXA. To our knowledge, this is the first cohort of patients with EM of PAS in whom coagulation monitoring and use of TXA have been shown to successfully treat hyperfibrinolysis.
Keywords: D-dimer; disseminated intravascular coagulopathy; expectant management; fibrinogen; hyperfibrinolysis; placenta accreta spectrum; tranexamic acid.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Conservative management of abnormally invasive placenta complicated by local hyperfibrinolysis and beginning disseminated intravascular coagulation.Arch Gynecol Obstet. 2021 Jan;303(1):61-68. doi: 10.1007/s00404-020-05721-0. Epub 2020 Aug 18. Arch Gynecol Obstet. 2021. PMID: 32809062 Free PMC article.
-
Risk of Subsequent Hysterectomy after Expectant Management in the Treatment of Placenta Accreta Spectrum Disorders.Medicina (Kaunas). 2022 May 19;58(5):678. doi: 10.3390/medicina58050678. Medicina (Kaunas). 2022. PMID: 35630092 Free PMC article. Review.
-
Uterine conservation in placenta accrete spectrum (PAS) disorders: A retrospective case series: Is expectant management beneficial in reducing maternal morbidity?Eur J Obstet Gynecol Reprod Biol. 2020 Nov;254:212-217. doi: 10.1016/j.ejogrb.2020.09.029. Epub 2020 Sep 24. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 33011503
-
Coagulopathy in surgical management of placenta accreta spectrum.Eur J Obstet Gynecol Reprod Biol. 2019 Jun;237:126-130. doi: 10.1016/j.ejogrb.2019.04.026. Epub 2019 Apr 19. Eur J Obstet Gynecol Reprod Biol. 2019. PMID: 31029971
-
Role of interventional radiology in pregnancy complicated by placenta accreta spectrum disorder: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2019 Jun;53(6):743-751. doi: 10.1002/uog.20131. Ultrasound Obstet Gynecol. 2019. PMID: 30255598
Cited by
-
Rectangular-Shaped Hemostatic Sutures in the Management of Second-Trimester Placenta Accreta Spectrum Disorders at Tu Du Hospital, Vietnam: A Retrospective Descriptive Study.AJP Rep. 2025 Jun 10;15(2):e79-e88. doi: 10.1055/a-2608-0990. eCollection 2025 Apr. AJP Rep. 2025. PMID: 40503449 Free PMC article.
References
-
- Sentilhes L., Kayem G., Chandraharan E., Palacios-Jaraquemada J., Jauniaux E. FIGO Placenta Accreta Diagnosis and Management Expert Consensus Panel FIGO Consensus Guidelines on Placenta Accreta Spectrum Disorders: Conservative Management. Int. J. Gynecol. Obstet. 2018;140:291–298. doi: 10.1002/ijgo.12410. - DOI - PubMed
LinkOut - more resources
Full Text Sources
