

Survival and Recurrence of Endocarditis following Mechanical vs. Biological Aortic Valve Replacement for Endocarditis in Patients Aged 40 to 65 Years: Data from the INFECT-Registry
- PMID: 38202159
- PMCID: PMC10779833
- DOI: 10.3390/jcm13010153
Survival and Recurrence of Endocarditis following Mechanical vs. Biological Aortic Valve Replacement for Endocarditis in Patients Aged 40 to 65 Years: Data from the INFECT-Registry
Abstract
Background: Infective endocarditis (IE) is a serious disease, and in many cases, surgery is necessary. Whether the type of prosthesis implanted for aortic valve replacement (AVR) for IE impacts patient survival is a matter of debate. The aim of the present study is to quantify differences in long-term survival and recurrence of endocarditis AVR for IE according to prosthesis type among patients aged 40 to 65 years.
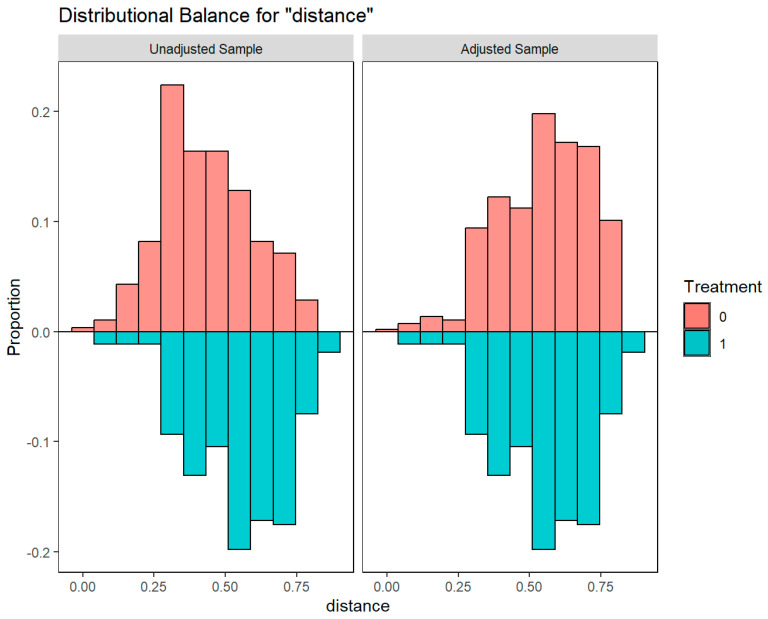
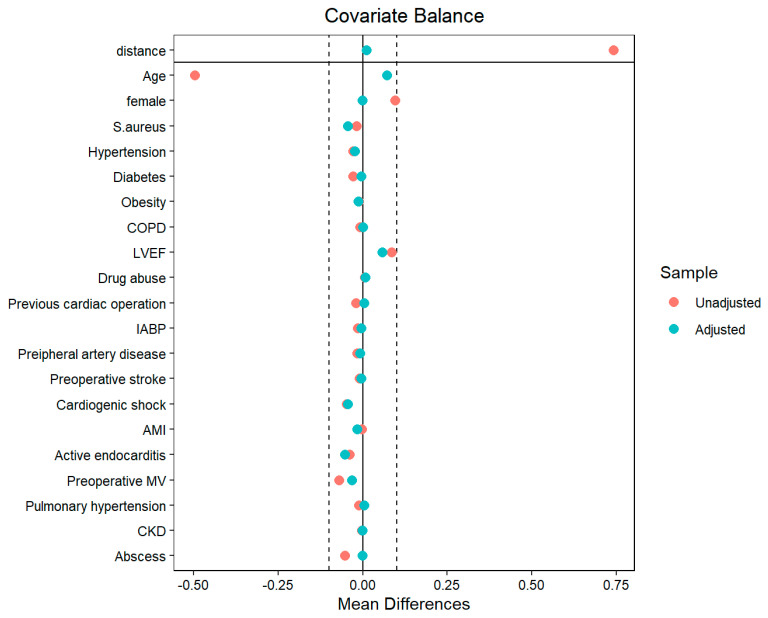
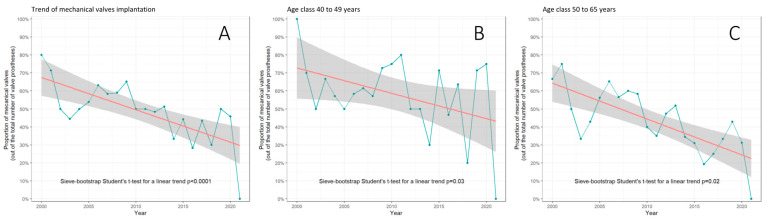
Methods: This was an analysis of the INFECT-REGISTRY. Trends in proportion to the use of mechanical prostheses versus biological ones over time were tested by applying the sieve bootstrapped t-test. Confounders were adjusted using the optimal full-matching propensity score. The difference in overall survival was compared using the Cox model, whereas the differences in recurrence of endocarditis were evaluated using the Gray test.
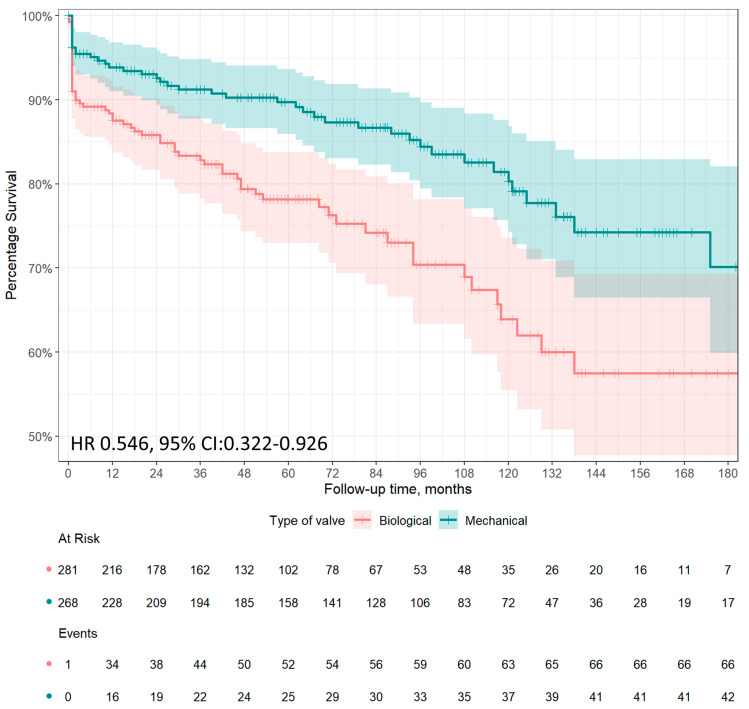
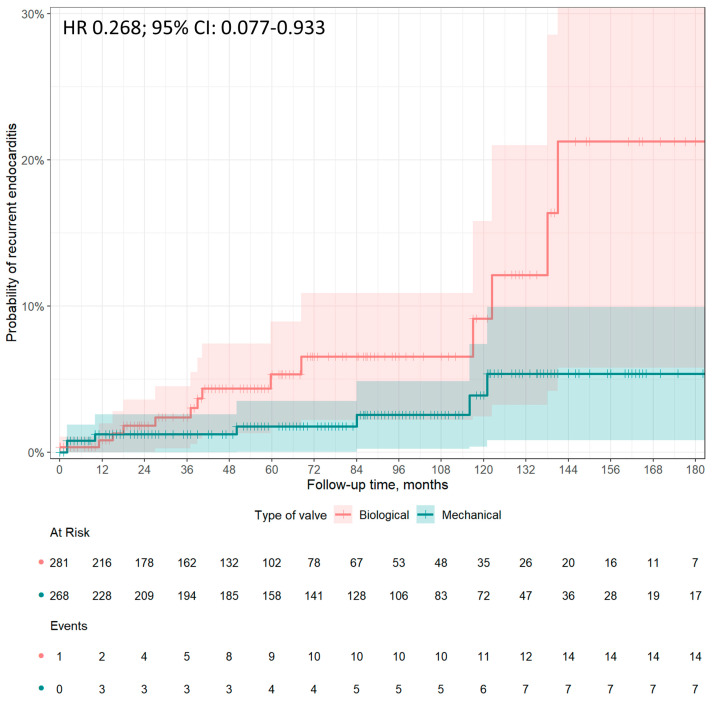
Results: Overall, 4365 patients were diagnosed and operated on for IE from 2000 to 2021. Of these, 549, aged between 40 and 65 years, underwent AVR. A total of 268 (48.8%) received mechanical prostheses, and 281 (51.2%) received biological ones. A significant trend in the reduction of implantation of mechanical vs. biological prostheses was observed during the study period (p < 0.0001). Long-term survival was significantly higher among patients receiving a mechanical prosthesis than those receiving a biological prosthesis (hazard ratio [HR] 0.546, 95% CI: 0.322-0.926, p = 0.025). Mechanical prostheses were associated with significantly less recurrent endocarditis after AVR than biological prostheses (HR 0.268, 95%CI: 0.077-0.933, p = 0.039).
Conclusions: The present analysis of the INFECT-REGISTRY shows increased survival and reduced recurrence of endocarditis after a mechanical aortic valve prosthesis implant for IE in middle-aged patients.
Keywords: aortic valve replacement; endocarditis; prosthetic heart valve.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Delahaye F., Chu V.H., Altclas J., Barsic B., Delahaye A., Freiberger T., Gordon D.L., Hannan M.M., Hoen B., Kanj S.S., et al. One-year outcome following biological or mechanical valve replacement for infective endocarditis. Int. J. Cardiol. 2015;78:117–123. doi: 10.1016/j.ijcard.2014.10.125. - DOI - PubMed
