

Safety and Feasibility of Intraoperative High PEEP Titrated to the Lowest Driving Pressure (ΔP)-Interim Analysis of DESIGNATION
- PMID: 38202214
- PMCID: PMC10780246
- DOI: 10.3390/jcm13010209
Safety and Feasibility of Intraoperative High PEEP Titrated to the Lowest Driving Pressure (ΔP)-Interim Analysis of DESIGNATION
Abstract
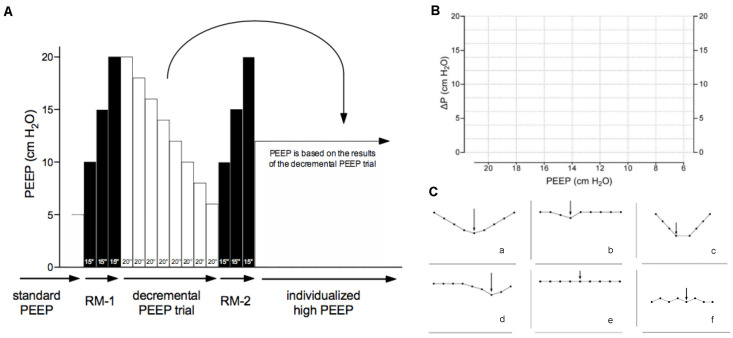
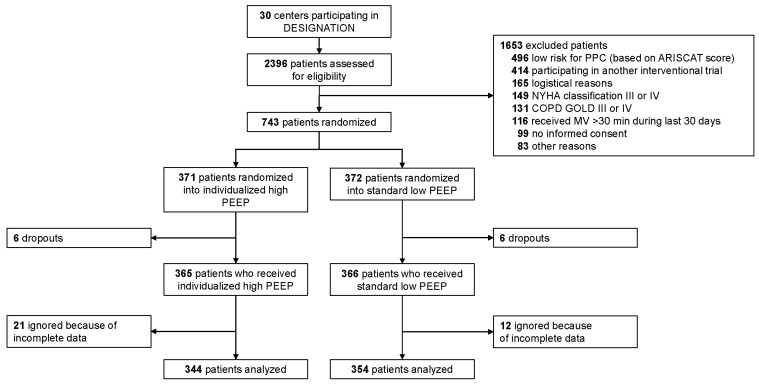
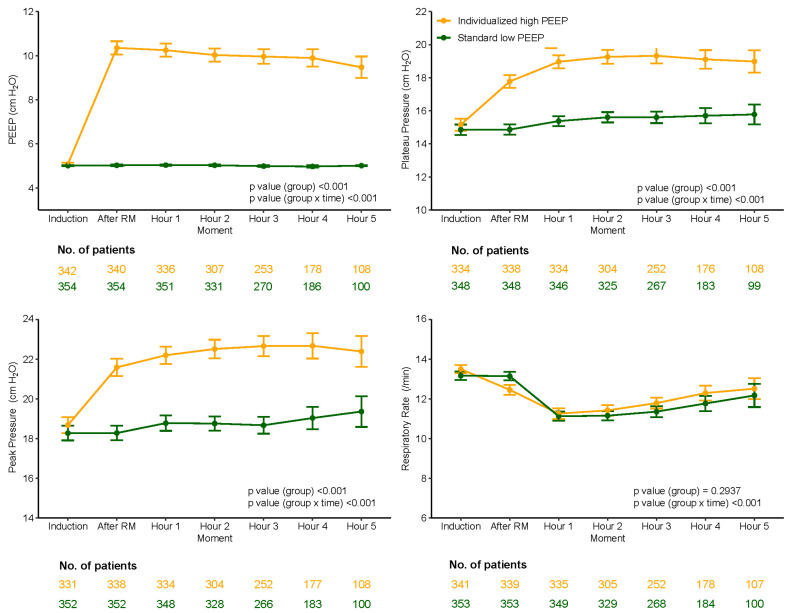
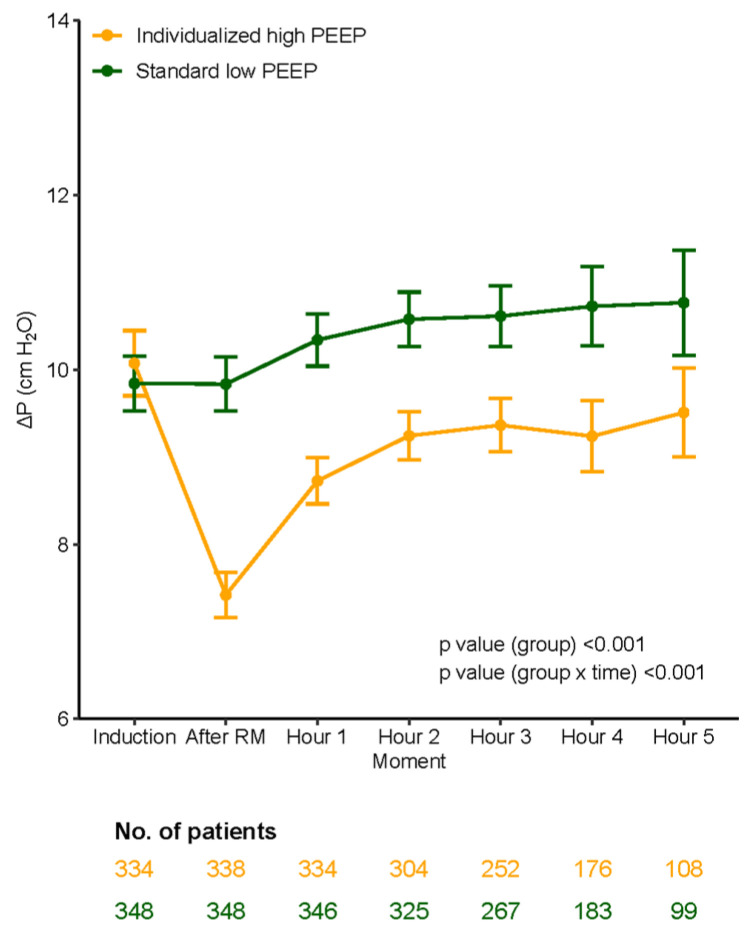
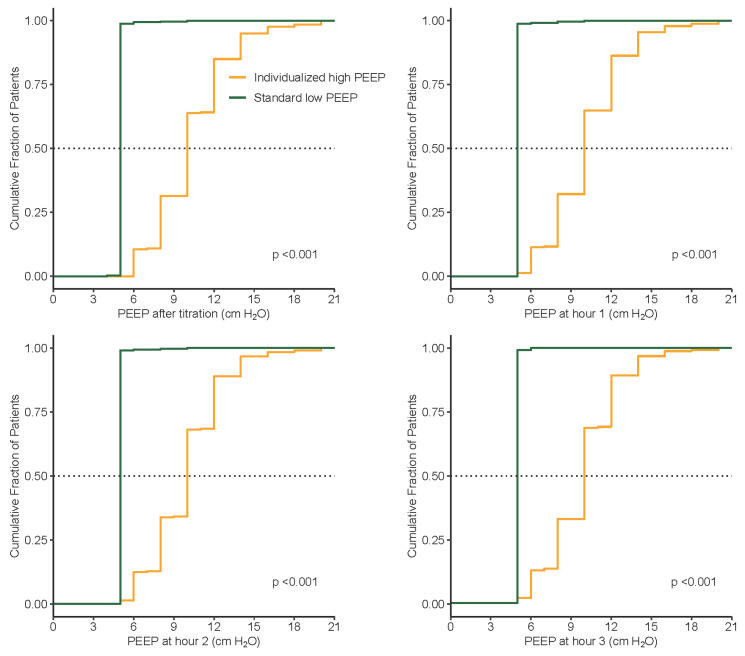
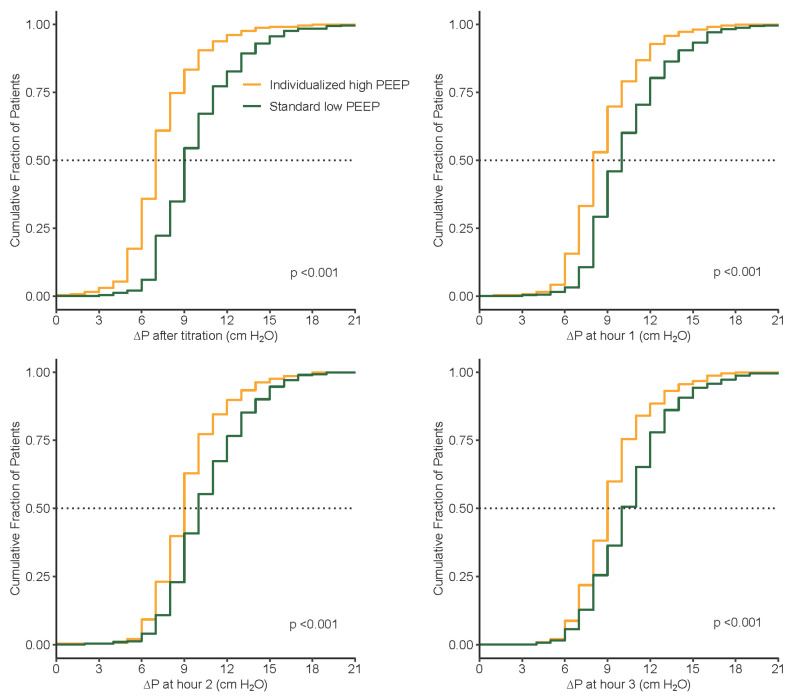
Uncertainty remains about the best level of intraoperative positive end-expiratory pressure (PEEP). An ongoing RCT ('DESIGNATION') compares an 'individualized high PEEP' strategy ('iPEEP')-titrated to the lowest driving pressure (ΔP) with recruitment maneuvers (RM), with a 'standard low PEEP' strategy ('low PEEP')-using 5 cm H2O without RMs with respect to the incidence of postoperative pulmonary complications. This report is an interim analysis of safety and feasibility. From September 2018 to July 2022, we enrolled 743 patients. Data of 698 patients were available for this analysis. Hypotension occurred more often in 'iPEEP' vs. 'low PEEP' (54.7 vs. 44.1%; RR, 1.24 (95% CI 1.07 to 1.44); p < 0.01). Investigators were compliant with the study protocol 285/344 patients (82.8%) in 'iPEEP', and 345/354 patients (97.5%) in 'low PEEP' (p < 0.01). Most frequent protocol violation was missing the final RM at the end of anesthesia before extubation; PEEP titration was performed in 99.4 vs. 0%; PEEP was set correctly in 89.8 vs. 98.9%. Compared to 'low PEEP', the 'iPEEP' group was ventilated with higher PEEP (10.0 (8.0-12.0) vs. 5.0 (5.0-5.0) cm H2O; p < 0.01). Thus, in patients undergoing general anesthesia for open abdominal surgery, an individualized high PEEP ventilation strategy is associated with hypotension. The protocol is feasible and results in clear contrast in PEEP. DESIGNATION is expected to finish in late 2023.
Keywords: PEEP; RM; anesthesia; driving pressure; feasibility; interim analysis; intraoperative ventilation; positive end–expiratory pressure; recruitment maneuver; safety; ventilation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Driving pressure during general anesthesia for minimally invasive abdominal surgery (GENERATOR)-study protocol of a randomized clinical trial.Trials. 2024 Oct 26;25(1):719. doi: 10.1186/s13063-024-08479-x. Trials. 2024. PMID: 39456048 Free PMC article.
-
Driving Pressure During General Anesthesia for Open Abdominal Surgery (DESIGNATION): study protocol of a randomized clinical trial.Trials. 2020 Feb 18;21(1):198. doi: 10.1186/s13063-020-4075-z. Trials. 2020. PMID: 32070400 Free PMC article.
-
Effects of intraoperative individualized PEEP on postoperative atelectasis in obese patients: study protocol for a prospective randomized controlled trial.Trials. 2020 Jul 6;21(1):618. doi: 10.1186/s13063-020-04565-y. Trials. 2020. PMID: 32631414 Free PMC article.
-
Effects of peep on lung injury, pulmonary function, systemic circulation and mortality in animals with uninjured lungs-a systematic review.Ann Transl Med. 2018 Jan;6(2):25. doi: 10.21037/atm.2017.12.05. Ann Transl Med. 2018. PMID: 29430442 Free PMC article. Review.
-
Impact of a positive end-expiratory pressure strategy on oxygenation, respiratory compliance, and hemodynamics during laparoscopic surgery in non-obese patients: a systematic review and meta-analysis of randomized controlled trials.BMC Anesthesiol. 2023 Nov 11;23(1):371. doi: 10.1186/s12871-023-02337-0. BMC Anesthesiol. 2023. PMID: 37950169 Free PMC article.
Cited by
-
Driving pressure during general anesthesia for minimally invasive abdominal surgery (GENERATOR)-study protocol of a randomized clinical trial.Trials. 2024 Oct 26;25(1):719. doi: 10.1186/s13063-024-08479-x. Trials. 2024. PMID: 39456048 Free PMC article.
References
-
- Hemmes S.N., Gama de Abreu M., Pelosi P., Schultz M.J. High versus low positive end-expiratory pressure during general anaesthesia for open abdominal surgery (PROVHILO trial): A multicentre randomised controlled trial. Lancet. 2014;384:495–503. doi: 10.1016/s0140-6736(14)60416-5. - DOI - PMC - PubMed
-
- Pereira S.M., Tucci M.R., Morais C.C.A., Simoes C.M., Tonelotto B.F.F., Pompeo M.S., Kay F.U., Pelosi P., Vieira J.E., Amato M.B.P. Individual Positive End-expiratory Pressure Settings Optimize Intraoperative Mechanical Ventilation and Reduce Postoperative Atelectasis. Anesthesiology. 2018;129:1070–1081. doi: 10.1097/ALN.0000000000002435. - DOI - PubMed
-
- Serpa Neto A., Barbas C.S.V., Simonis F.D., Artigas-Raventós A., Canet J., Determann R.M., Anstey J., Hedenstierna G., Hemmes S.N.T., Hermans G., et al. Epidemiological characteristics, practice of ventilation, and clinical outcome in patients at risk of acute respiratory distress syndrome in intensive care units from 16 countries (PRoVENT): An international, multicentre, prospective study. Lancet Respir. Med. 2016;4:882–893. doi: 10.1016/S2213-2600(16)30305-8. - DOI - PubMed
-
- Serpa Neto A., Amato M.B.P., Schultz M.J. Dissipated Energy is a Key Mediator of VILI: Rationale for Using Low Driving Pressures. In: Vincent J.-L., editor. Annual Update in Intensive Care and Emergency Medicine 2016. Springer International Publishing; Cham, Switzerland: 2016. pp. 311–321.
Grants and funding
LinkOut - more resources
Full Text Sources
