

Diabetes Status, c-Reactive Protein, and Insulin Resistance in Community-Acquired Pneumonia-A Prospective Cohort Study
- PMID: 38202252
- PMCID: PMC10780000
- DOI: 10.3390/jcm13010245
Diabetes Status, c-Reactive Protein, and Insulin Resistance in Community-Acquired Pneumonia-A Prospective Cohort Study
Abstract
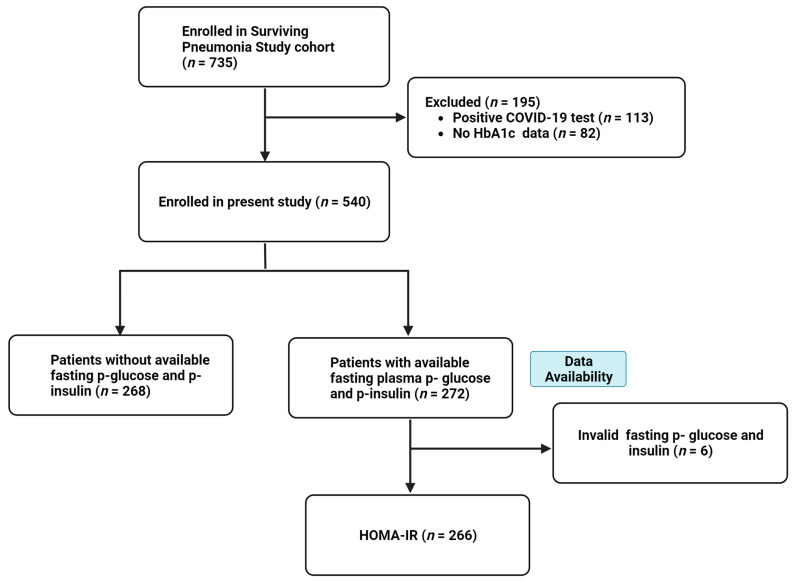
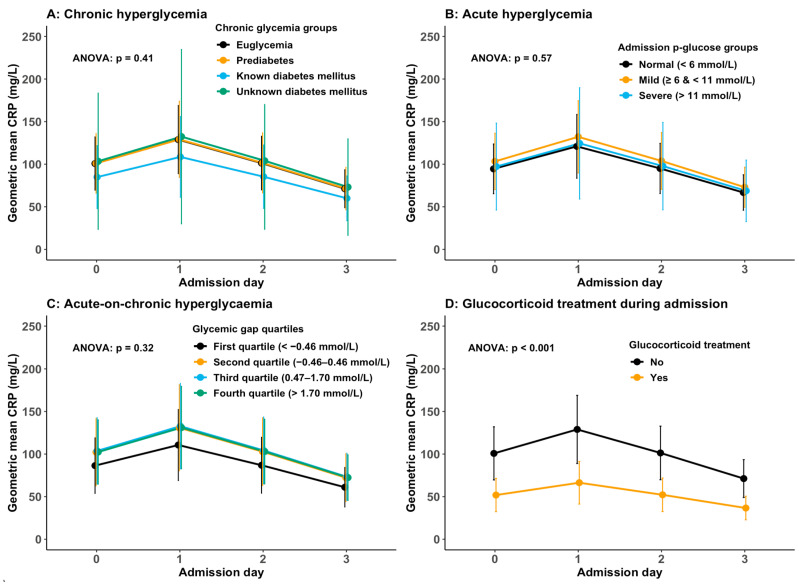
C-reactive protein (CRP) is commonly used to guide community-acquired pneumonia (CAP) treatment. A positive association between admission glucose and CRP levels has been observed in patients with CAP. The associations between prediabetes, unknown diabetes, acute-on-chronic hyperglycaemia, and CRP levels, and between admission CRP levels and insulin resistance (IR) in CAP, remain unexplored. This study investigated the associations firstly between chronic, acute, and acute-on-chronic hyperglycaemia and CRP levels, and secondly between admission CRP levels and IR in CAP. In a prospective cohort study of adults with CAP, the associations between chronic, acute, and acute-on-chronic hyperglycaemia (admission glucose minus HbA1c-derived average glucose) and CRP levels until admission day 3 were modelled with repeated-measures linear mixed models. IR was estimated with the homeostasis model assessment of IR (HOMA-IR). The association between admission CRP levels and HOMA-IR was modelled with linear regression. In 540 patients, no association between chronic, acute, or acute-on-chronic hyperglycaemia and CRP levels was found. In 266 patients, every 50 mg/L increase in admission CRP was associated with a 7% (95% CI 1-14%) higher HOMA-IR. In conclusion, our findings imply that hyperglycaemia does not influence CRP levels in patients with CAP, although admission CRP levels were positively associated with IR.
Keywords: acute hyperglycaemia; acute-on-chronic hyperglycaemia; c-reactive protein; chronic hyperglycaemia; community-acquired pneumonia; diabetes mellitus; insulin resistance.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pletz M.W., Jensen A.V., Bahrs C., Davenport C., Rupp J., Witzenrath M., Barten-Neiner G., Kolditz M., Dettmer S., Chalmers J.D., et al. Unmet needs in pneumonia research: A comprehensive approach by the CAPNETZ study group. Respir. Res. 2022;23:239. doi: 10.1186/s12931-022-02117-3. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
