

Pathogenic Variant Frequencies in Hereditary Haemorrhagic Telangiectasia Support Clinical Evidence of Protection from Myocardial Infarction
- PMID: 38202257
- PMCID: PMC10779873
- DOI: 10.3390/jcm13010250
Pathogenic Variant Frequencies in Hereditary Haemorrhagic Telangiectasia Support Clinical Evidence of Protection from Myocardial Infarction
Abstract
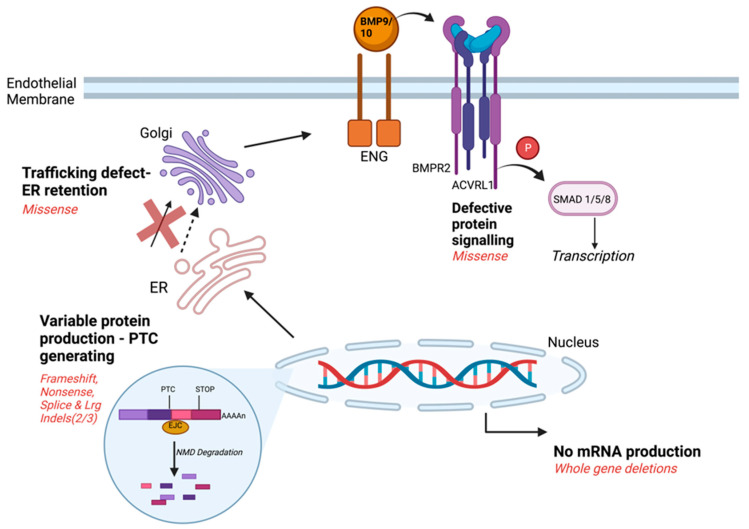
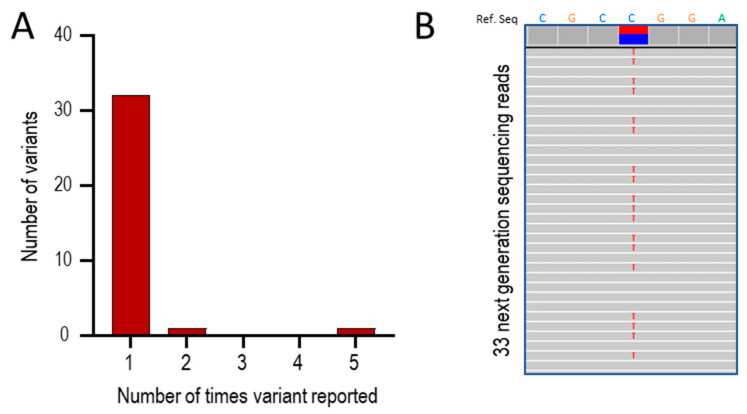
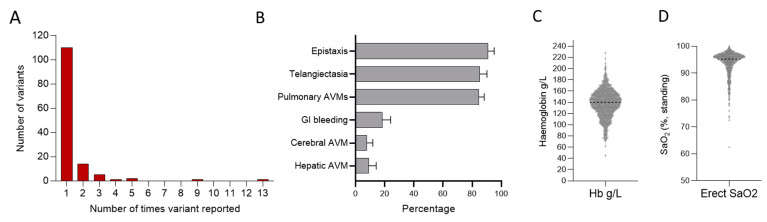
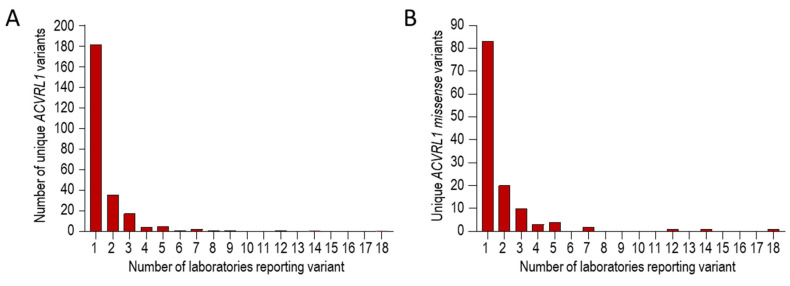
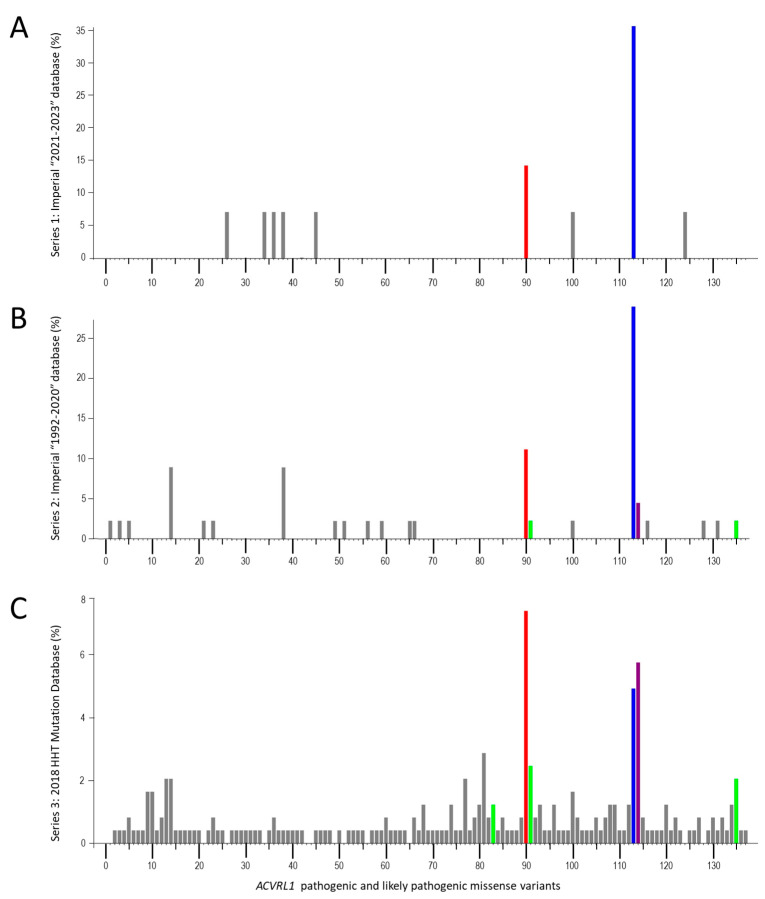
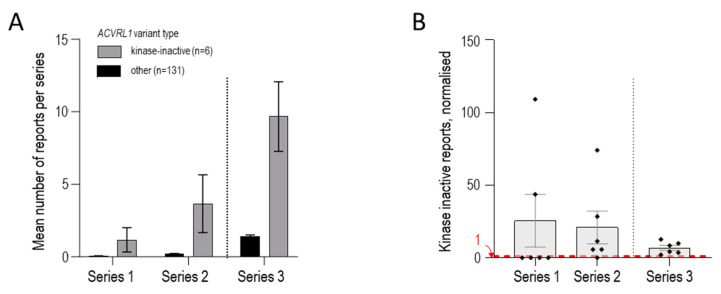
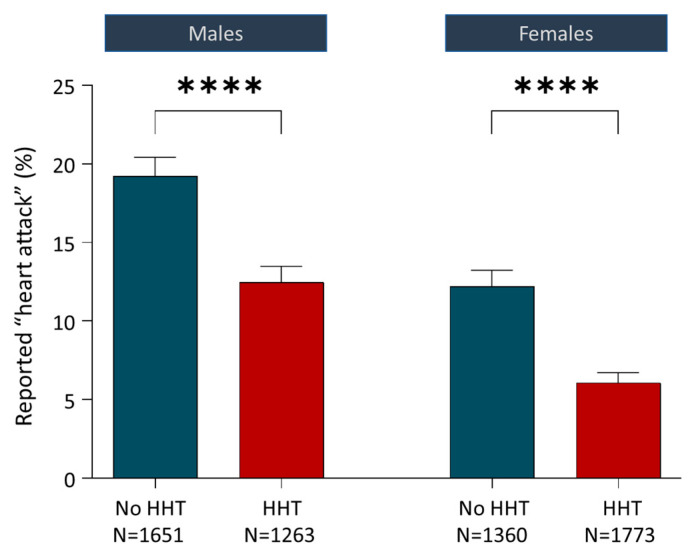
Hereditary haemorrhagic telangiectasia (HHT) is a vascular dysplasia inherited as an autosomal dominant trait, due to a single heterozygous loss-of-function variant, usually in ACVRL1 (encoding activin receptor-like kinase 1 [ALK1]), ENG (encoding endoglin [CD105]), or SMAD4. In a consecutive single-centre series of 37 positive clinical genetic tests performed in 2021-2023, a skewed distribution pattern was noted, with 30 of 32 variants reported only once, but ACVRL1 c.1231C>T (p.Arg411Trp) identified as the disease-causal gene in five different HHT families. In the same centre's non-overlapping 1992-2020 series where 110/134 (82.1%) HHT-causal variants were reported only once, ACVRL1 c.1231C>T (p.Arg411Trp) was identified in nine further families. In a 14-country, four-continent HHT Mutation Database where 181/250 (72.4%) HHT-causal variants were reported only once, ACVRL1 c.1231C>T (p.Arg411Trp) was reported by 12 different laboratories, the adjacent ACVRL1 c.1232G>A (p.Arg411Gln) by 14, and ACVRL1 c.1120C>T (p.Arg374Trp) by 18. Unlike the majority of HHT-causal ACVRL1 variants, these encode ALK1 protein that reaches the endothelial cell surface but fails to signal. Six variants of this type were present in the three series and were reported 6.8-25.5 (mean 8.9) times more frequently than the other ACVRL1 missense variants (all p-values < 0.0039). Noting lower rates of myocardial infarction reported in HHT, we explore potential mechanisms, including a selective paradigm relevant to ALK1's role in the initiating event of atherosclerosis, where a plausible dominant negative effect of these specific variants can be proposed. In conclusion, there is an ~9-fold excess of kinase-inactive, cell surface-expressed ACVRL1/ALK1 pathogenic missense variants in HHT. The findings support further examination of differential clinical and cellular phenotypes by HHT causal gene molecular subtypes.
Keywords: atherosclerosis; dominant negative activity; heart attack; low-density lipoprotein (LDL) transcytosis; missense variant.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Distribution of Cerebrovascular Phenotypes According to Variants of the ENG and ACVRL1 Genes in Subjects with Hereditary Hemorrhagic Telangiectasia.J Clin Med. 2022 May 10;11(10):2685. doi: 10.3390/jcm11102685. J Clin Med. 2022. PMID: 35628811 Free PMC article.
-
Molecular screening of ALK1/ACVRL1 and ENG genes in hereditary hemorrhagic telangiectasia in France.Hum Mutat. 2004 Apr;23(4):289-99. doi: 10.1002/humu.20017. Hum Mutat. 2004. PMID: 15024723
-
Mutational and clinical spectrum of Japanese patients with hereditary hemorrhagic telangiectasia.BMC Med Genomics. 2021 Dec 6;14(1):288. doi: 10.1186/s12920-021-01139-y. BMC Med Genomics. 2021. PMID: 34872578 Free PMC article.
-
Endoglin and alk1 as therapeutic targets for hereditary hemorrhagic telangiectasia.Expert Opin Ther Targets. 2017 Oct;21(10):933-947. doi: 10.1080/14728222.2017.1365839. Epub 2017 Aug 20. Expert Opin Ther Targets. 2017. PMID: 28796572 Review.
-
An update on preclinical models of hereditary haemorrhagic telangiectasia: Insights into disease mechanisms.Front Med (Lausanne). 2022 Sep 29;9:973964. doi: 10.3389/fmed.2022.973964. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36250069 Free PMC article. Review.
Cited by
-
National Guidelines for Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Peritoneal Malignancies: A Worldwide Systematic Review and Recommendations of Strength Analysis.Ann Surg Oncol. 2025 Aug;32(8):5795-5806. doi: 10.1245/s10434-025-17518-z. Epub 2025 May 24. Ann Surg Oncol. 2025. PMID: 40413333 Free PMC article.
-
Hereditary haemorrhagic telangiectasia.Nat Rev Dis Primers. 2025 Jan 9;11(1):1. doi: 10.1038/s41572-024-00585-z. Nat Rev Dis Primers. 2025. PMID: 39788978 Review.
-
Mutations causing premature termination codons discriminate and generate cellular and clinical variability in HHT.Blood. 2024 May 30;143(22):2314-2331. doi: 10.1182/blood.2023021777. Blood. 2024. PMID: 38457357 Free PMC article.
-
Decoding clinical diversity in monogenic TGFBR1 and TGFBR2 mutations: insights into the interplay of molecular mechanisms and hypomorphicity.Front Cell Dev Biol. 2025 Jun 19;13:1580274. doi: 10.3389/fcell.2025.1580274. eCollection 2025. Front Cell Dev Biol. 2025. PMID: 40612107 Free PMC article. Review.
-
When "loss-of-function" means proteostasis burden: Thinking again about coding DNA variants.Am J Hum Genet. 2025 Jan 2;112(1):3-10. doi: 10.1016/j.ajhg.2024.12.002. Am J Hum Genet. 2025. PMID: 39753117 Free PMC article.
References
-
- Legg W. A case of Haemophilia complicated with Multiple Naevi. Lancet. 1876;2:856–857.
-
- Sutton H.G. Epistaxis as an indication of impaired nutrition, and of degeneration of the vascular system. Med. Mirror. 1864;1:769–781.
-
- Babington B.G. Hereditary epistaxis. Lancet. 1865;86:362–363.
-
- Rendu H. Épistaxis répetées chez un sujet porteur de petits angiomes cutanés et muquez. Gaz. Des. Hop. 1896;135:1322–1323.
-
- Osler W. On a family form of recurring epistaxis, associated with multiple telangiectases of the skin and mucous membranes. Bull. Johns Hopkins Hosp. 1901;12:333–337.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
