

Aortic Vascular Graft and Endograft Infection-Patient Outcome Cannot Be Determined Based on Pre-Operative Characteristics
- PMID: 38202276
- PMCID: PMC10779700
- DOI: 10.3390/jcm13010269
Aortic Vascular Graft and Endograft Infection-Patient Outcome Cannot Be Determined Based on Pre-Operative Characteristics
Abstract
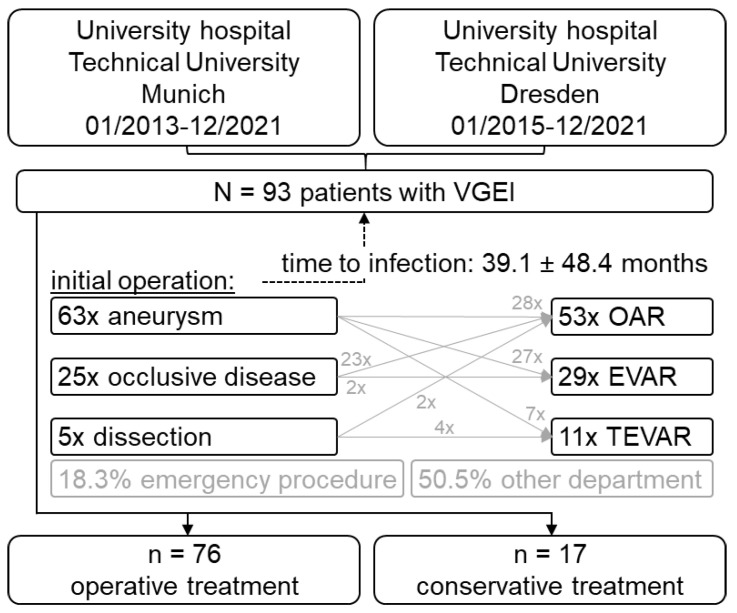
Vascular graft/endograft infection (VGEI) is a serious complication after aortic surgery. This study investigates VGEI and patient characteristics, PET/CT quantification before surgical or conservative management of VGEI and post-intervention outcomes in order to identify patients who might benefit from such a procedure. PET standard uptake values (SUV) were quantitatively assessed and compared to a non-VGEI cohort. The primary endpoints were in-hospital mortality and aortic reintervention-free survival at six months. Ninety-three patients (75% male, 65 ± 10 years, 82% operated) were included. The initial operation was mainly for aneurysm (67.7%: 31% EVAR, 12% TEVAR, 57% open aortic repair). Thirty-two patients presented with fistulae. PET SUVTLR (target-to-liver ratio) showed 94% sensitivity and 89% specificity. Replacement included silver-coated Dacron (21.3%), pericardium (61.3%) and femoral vein (17.3%), yet the material did not influence the overall survival (p = 0.745). In-hospital mortality did not differ between operative and conservative treatment (19.7% vs. 17.6%, p = 0.84). At six months, 50% of the operated cohort survived without aortic reintervention. Short- and midterm morbidity and mortality remained high after aortic graft removal. Neither preoperative characteristics nor the material used for reconstruction influenced the overall survival, and, with limitations, both the in-hospital and midterm survival were similar between the surgically and conservatively managed patients.
Keywords: aortic graft infection; pericardial prosthesis; silver graft; vascular graft endograft infection.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
The relevance of aortic endograft prosthetic infection.J Vasc Surg. 2011 Aug;54(2):327-33. doi: 10.1016/j.jvs.2010.12.067. Epub 2011 Mar 11. J Vasc Surg. 2011. PMID: 21397443
-
Reconstruction of primary and secondary aortic infections with an antimicrobial graft.J Vasc Surg. 2023 Apr;77(4):1226-1237.e10. doi: 10.1016/j.jvs.2022.11.065. Epub 2022 Dec 23. J Vasc Surg. 2023. PMID: 36572322
-
Conservative Management First Strategy in Aortic Vascular Graft and Endograft Infections.Eur J Vasc Endovasc Surg. 2023 Jun;65(6):896-904. doi: 10.1016/j.ejvs.2023.03.003. Epub 2023 Mar 13. Eur J Vasc Endovasc Surg. 2023. PMID: 36921753
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
-
Endograft Infection After Endovascular Abdominal Aortic Aneurysm Repair: A Systematic Review and Meta-analysis.J Endovasc Ther. 2017 Oct;24(5):688-697. doi: 10.1177/1526602817722018. Epub 2017 Jul 31. J Endovasc Ther. 2017. PMID: 28756719
References
-
- Wanhainen A., Verzini F., Van Herzeele I., Allaire E., Bown M., Cohnert T., Dick F., van Herwaarden J., Karkos C., Koelemay M., et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019;57:8–93. doi: 10.1016/j.ejvs.2018.09.020. - DOI - PubMed
-
- Lyons O.T., Baguneid M., Barwick T.D., Bell R.E., Foster N., Homer-Vanniasinkam S., Hopkins S., Hussain A., Katsanos K., Modarai B., et al. Diagnosis of Aortic Graft Infection: A Case Definition by the Management of Aortic Graft Infection Collaboration (MAGIC) Eur. J. Vasc. Endovasc. Surg. 2016;52:758–763. doi: 10.1016/j.ejvs.2016.09.007. - DOI - PubMed
-
- Chakfe N., Diener H., Lejay A., Assadian O., Berard X., Caillon J., Fourneau I., Glaudemans A., Koncar I., Lindholt J., et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Vascular Graft and Endograft Infections. Eur. J. Vasc. Endovasc. Surg. 2020;59:339–384. doi: 10.1016/j.ejvs.2019.10.016. - DOI - PubMed
-
- Anagnostopoulos A., Mayer F., Ledergerber B., Bergada-Pijuan J., Husmann L., Mestres C.A., Rancic Z., Hasse B., Study V.C. Editor’s Choice—Validation of the Management of Aortic Graft Infection Collaboration (MAGIC) Criteria for the Diagnosis of Vascular Graft/Endograft Infection: Results from the Prospective Vascular Graft Cohort Study. Eur. J. Vasc. Endovasc. Surg. 2021;62:251–257. doi: 10.1016/j.ejvs.2021.05.010. - DOI - PubMed
-
- Dong W., Li Y., Zhu J., Xia J., He L., Yun M., Jiao J., Zhu G., Hacker M., Wei Y., et al. Detection of aortic prosthetic graft infection with 18F-FDG PET/CT imaging, concordance with consensus MAGIC graft infection criteria. J. Nucl. Cardiol. 2021;28:1005–1016. doi: 10.1007/s12350-020-02227-9. - DOI - PubMed
LinkOut - more resources
Full Text Sources
