

Pan-EGFR Inhibitor Dacomitinib Resensitizes Paclitaxel and Induces Apoptosis via Elevating Intracellular ROS Levels in Ovarian Cancer SKOV3-TR Cells
- PMID: 38202856
- PMCID: PMC10780346
- DOI: 10.3390/molecules29010274
Pan-EGFR Inhibitor Dacomitinib Resensitizes Paclitaxel and Induces Apoptosis via Elevating Intracellular ROS Levels in Ovarian Cancer SKOV3-TR Cells
Abstract
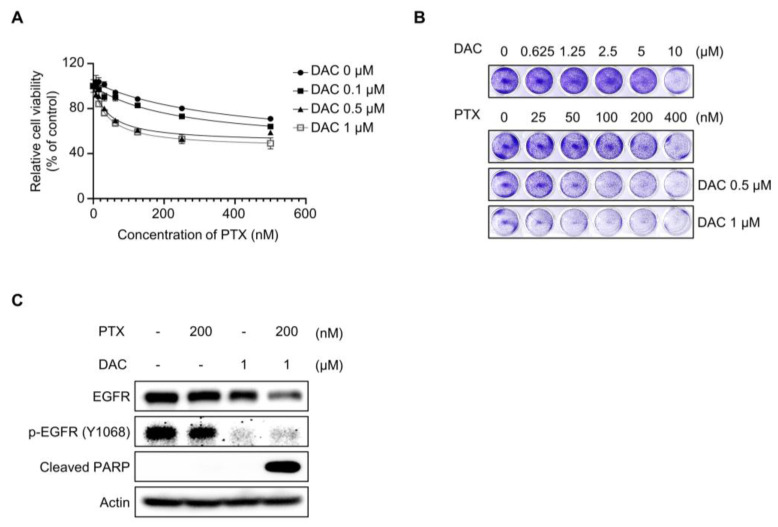
Paclitaxel is still used as a standard first-line treatment for ovarian cancer. Although paclitaxel is effective for many types of cancer, the emergence of chemoresistant cells represents a major challenge in chemotherapy. Our study aimed to analyze the cellular mechanism of dacomitinib, a pan-epidermal growth factor receptor (EGFR) inhibitor, which resensitized paclitaxel and induced cell cytotoxicity in paclitaxel-resistant ovarian cancer SKOV3-TR cells. We investigated the significant reduction in cell viability cotreated with dacomitinib and paclitaxel by WST-1 assay and flow cytometry analysis. Dacomitinib inhibited EGFR family proteins, including EGFR and HER2, as well as its downstream signaling proteins, including AKT, STAT3, ERK, and p38. In addition, dacomitinib inhibited the phosphorylation of Bad, and combination treatment with paclitaxel effectively suppressed the expression of Mcl-1. A 2'-7'-dichlorodihydrofluorescein diacetate (DCFH-DA) assay revealed a substantial elevation in cellular reactive oxygen species (ROS) levels in SKOV3-TR cells cotreated with dacomitinib and paclitaxel, which subsequently mediated cell cytotoxicity. Additionally, we confirmed that dacomitinib inhibits chemoresistance in paclitaxel-resistant ovarian cancer HeyA8-MDR cells. Collectively, our research indicated that dacomitinib effectively resensitized paclitaxel in SKOV3-TR cells by inhibiting EGFR signaling and elevating intracellular ROS levels.
Keywords: dacomitinib; ovarian cancer; paclitaxel-resistance; pan-EGFR inhibitor; reactive oxygen species.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






Similar articles
-
Deguelin Restores Paclitaxel Sensitivity in Paclitaxel-Resistant Ovarian Cancer Cells via Inhibition of the EGFR Signaling Pathway.Cancer Manag Res. 2024 May 28;16:507-525. doi: 10.2147/CMAR.S457221. eCollection 2024. Cancer Manag Res. 2024. PMID: 38827785 Free PMC article.
-
Dacomitinib, a new pan-EGFR inhibitor, is effective in killing ovarian cancer cells.Discov Med. 2016 Nov;22(122):297-309. Discov Med. 2016. PMID: 28009971
-
Inhibition of Glutamine Uptake Resensitizes Paclitaxel Resistance in SKOV3-TR Ovarian Cancer Cell via mTORC1/S6K Signaling Pathway.Int J Mol Sci. 2022 Aug 6;23(15):8761. doi: 10.3390/ijms23158761. Int J Mol Sci. 2022. PMID: 35955892 Free PMC article.
-
Clinical evaluation of dacomitinib for the treatment of metastatic non-small cell lung cancer (NSCLC): current perspectives.Drug Des Devel Ther. 2019 Sep 6;13:3187-3198. doi: 10.2147/DDDT.S194231. eCollection 2019. Drug Des Devel Ther. 2019. PMID: 31564835 Free PMC article. Review.
-
Dacomitinib, a second-generation irreversible epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) to treat non-small cell lung cancer.Drugs Today (Barc). 2019 Apr;55(4):231-236. doi: 10.1358/dot.2019.55.4.2965337. Drugs Today (Barc). 2019. PMID: 31050691 Review.
References
-
- Matulonis U.A., Penson R.T., Domchek S.M., Kaufman B., Shapira-Frommer R., Audeh M.W., Kaye S., Molife L.R., Gelmon K.A., Robertson J.D., et al. Olaparib monotherapy in patients with advanced relapsed ovarian cancer and a germline BRCA1/2 mutation: A multistudy analysis of response rates and safety. Ann. Oncol. 2016;27:1013–1019. doi: 10.1093/annonc/mdw133. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
