

The robustness of the flow-gradient classification of severe aortic stenosis
- PMID: 38204672
- PMCID: PMC10775038
- DOI: 10.1016/j.xjon.2023.08.022
The robustness of the flow-gradient classification of severe aortic stenosis
Abstract
Objectives: A flow-gradient classification is used to determine the indication for intervention for patients with severe aortic stenosis (AS) with discordant echocardiographic parameters. We investigated the agreement in flow-gradient classification by stroke volume (SV) measurement at the left ventricular outflow tract (LVOT) and at the left ventricle.
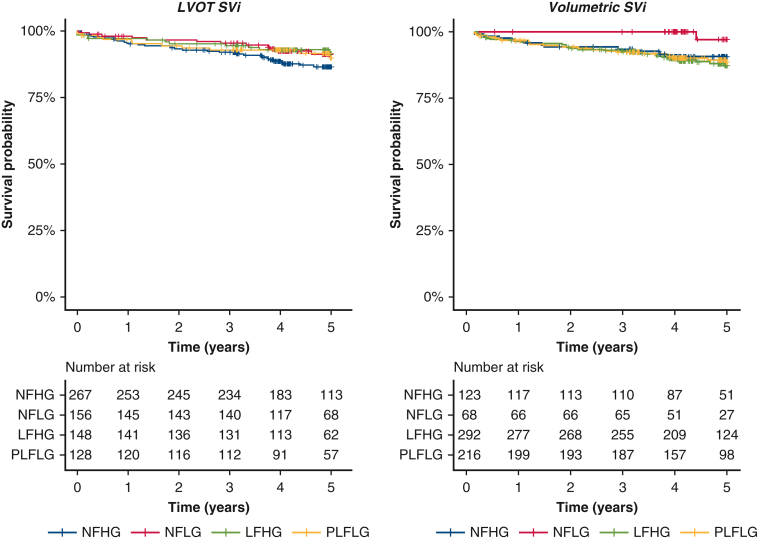
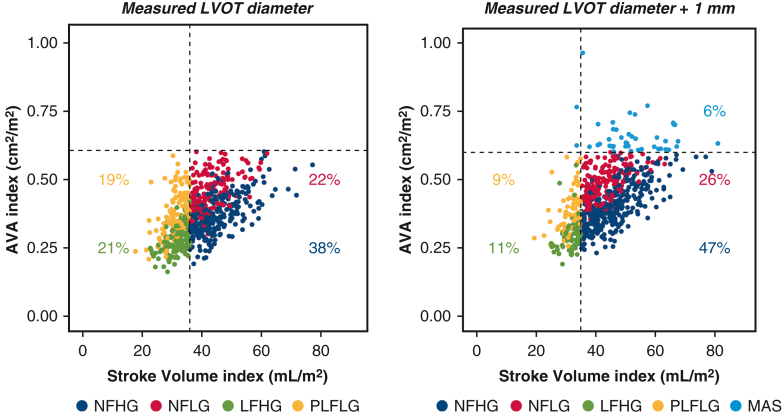
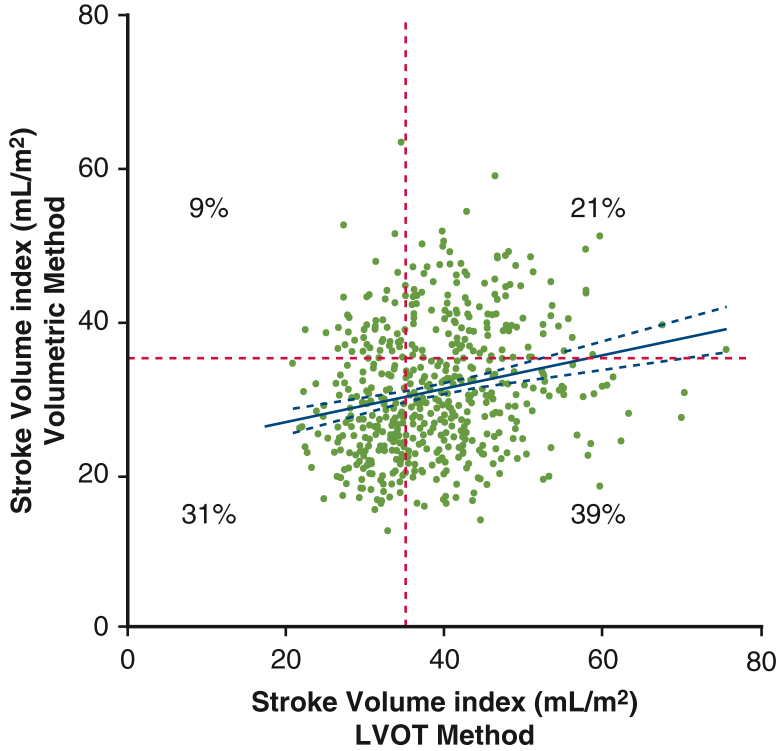
Methods: Data were used from a prospective cohort study and patients with severe AS (aortic valve area index ≤0.6 cm2/m2) with preserved ejection fraction (>50%) were selected. SV was determined by an echocardiographic core laboratory at the LVOT and by subtracting the 2-dimensional left ventricle end-systolic from the end-diastolic volume (volumetric). Patients were stratified into 4 groups based on SV index (35 mL/m2) and mean gradient (40 mm Hg). The group composition was compared and the agreement between the SV measurements was investigated using regression, correlation, and limits of agreement. In addition, a systematic LVOT diameter overestimation of 1 mm was simulated to study flow-gradient reclassification.
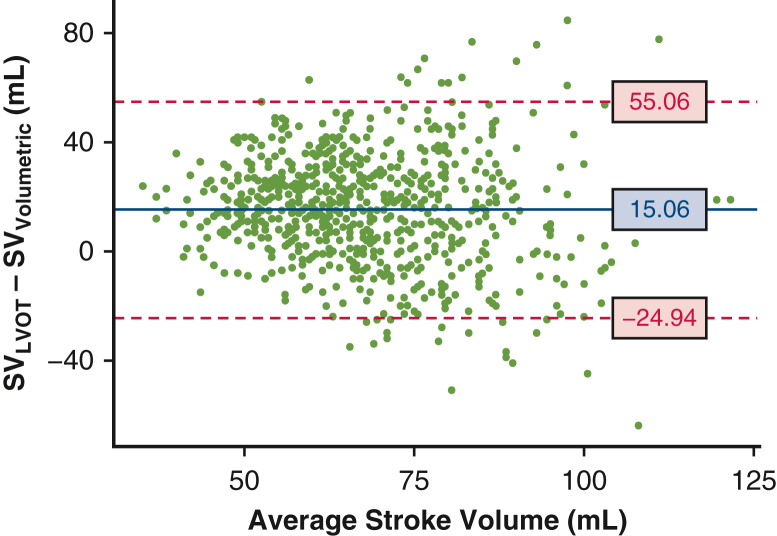
Results: Of 1118 patients, 699 were eligible. The group composition changed considerably as agreement on flow state occurred in only 50% of the measurements. LVOT SV was on average 15.1 mL (95% limits of agreement -24.9:55.1 mL) greater than volumetric SV. When a systematic 1-mm LVOT diameter overestimation was introduced, the low-flow groups halved.
Conclusions: There was poor agreement in the flow-gradient classification of severe AS as a result of large differences between LVOT and volumetric SV. Furthermore, this classification was sensitive to small measurement errors. These results stress that parameters beyond the flow-gradient classification should be considered to ensure accurate recommendations for intervention.
Keywords: flow-gradient classification; low flow; severe aortic stenosis; stroke volume.
© 2023 The Author(s).
Conflict of interest statement
B.V.: institutional research grant and speaker's honorarium paid to his department from Medtronic. M.V.: institutional research grant and reimbursement of travel expenses from Medtronic. F.A.: no personal conflicts of interest, but his organization receives grants or research contracts from Medtronic, Abbott, Edwards Lifesciences, Boston Scientific, Biotronik, Corcym, and HLT Medical. M.M.: trainer and consultant for Medtronic; a trainer and speaker for AtriCure; and a speaker and consultant for Haemonetics. F.D.: proctor and speaker for Medtronic and Cook Medical. M.R.: consultant to Medtronic, Abbott Medical, Boston Scientific, Gore Medical, and Transverse Medical; the fees are paid to his department. J.S.: Principal Investigator, PERIGON Pivotal Trial for Medtronic. R.K.: research support, consultation fees, and Principal Investigator, PERIGON Pivotal Trial for Medtronic. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures








References
-
- Baumgartner H., Hung J., Bermejo J., Chambers J.B., Edvardsen T., Goldstein S., et al. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. 2017;30:372–392. - PubMed
-
- Otto C.M., Nishimura R.A., Bonow R.O., Carabello B.A., Erwin J.P., III, Gentile F., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2021;143:e35–e71. - PubMed
-
- Vahanian A., Beyersdorf F., Praz F., Milojevic M., Baldus S., Bauersachs J., et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561–632. - PubMed
-
- Pibarot P., Dumesnil J.G. Paradoxical low-flow, low-gradient aortic stenosis: new evidence, more questions. Circulation. 2013;128:1729–1732. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
