

Risk of developing subsequent primary lung cancer after receiving radiation for breast cancer
- PMID: 38204675
- PMCID: PMC10775166
- DOI: 10.1016/j.xjon.2023.10.031
Risk of developing subsequent primary lung cancer after receiving radiation for breast cancer
Abstract
Background: Radiotherapy (RT) is integral to breast cancer treatment, especially in the current era that emphasizes breast conservation. The aim of our study was to determine the incidence of subsequent primary lung cancer after RT exposure for breast cancer over a time span of 3 decades to quantify this risk over time as modern oncologic treatment continues to evolve.
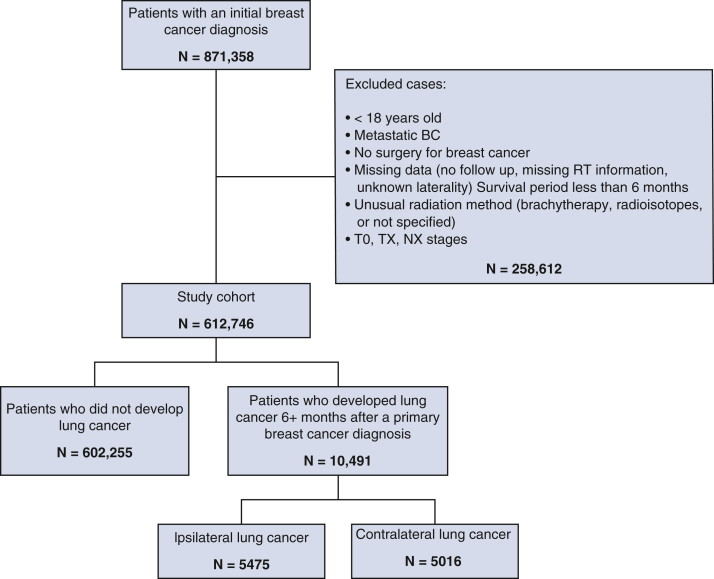
Methods: The SEER (Surveillance, Epidemiology, and End Results) database was queried from 1988 to 2014 for patients diagnosed with nonmetastatic breast cancer. Patients who subsequently developed primary lung cancer were identified. Multivariable regression modeling was performed to identify independent factors associated with the development of lung cancer stratified by follow up intervals of 5 to 9 years, 10 to 15 years, and >15 years after breast cancer diagnosis.
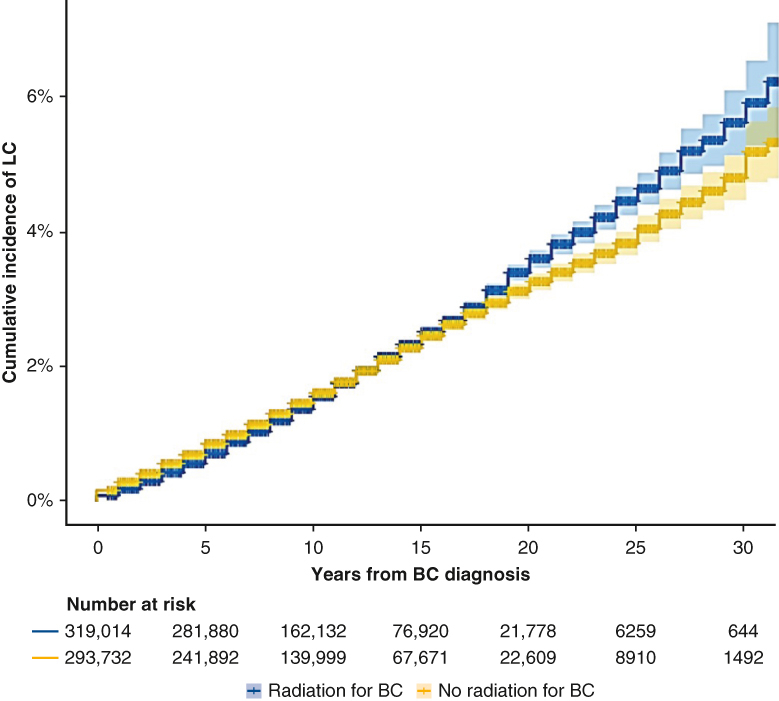
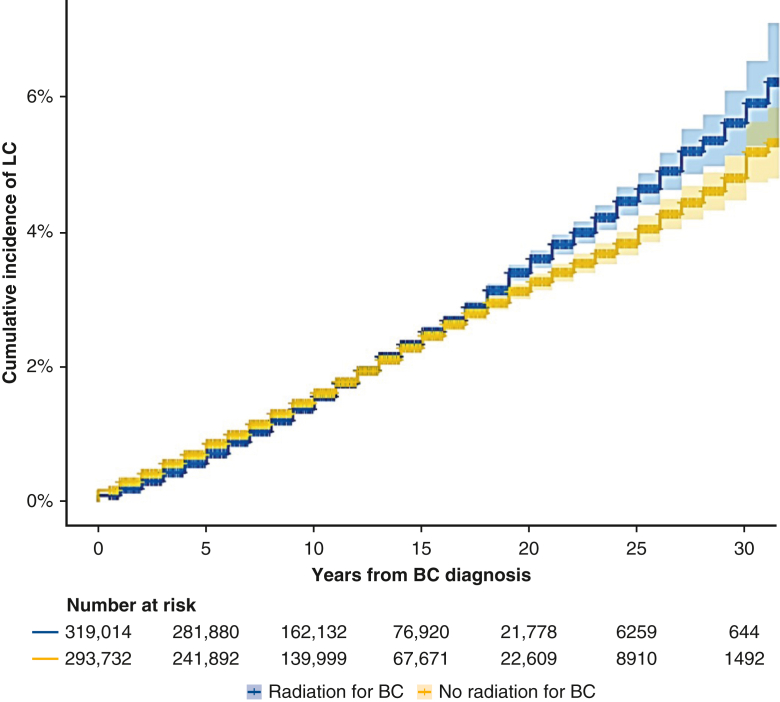
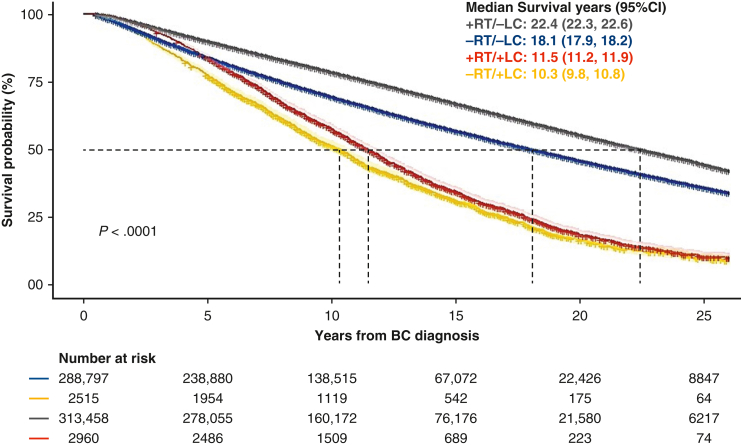
Results: Of the 612,746 patients who met our inclusion criteria, 319,014 (52%) were irradiated. primary lung cancer developed in 5556 patients (1.74%) in the RT group versus 4935 patients (1.68%) in the non-RT group. In a multivariable model stratified by follow-up duration, the overall HR of developing subsequent ipsilateral lung cancer in the RT group was 1.14 (P = .036) after 5 to 9 years of follow-up, 1.28 (P = .002) after 10 to 15 years of follow-up, and 1.30 (P = .014) after >15 years of follow-up. The HR of contralateral lung cancer was not increased at any time interval.
Conclusions: The increased risk of developing a primary lung cancer secondary to RT exposure for breast cancer is much lower than previously published. Modern RT techniques may have contributed to the improved risk profile, and this updated study is important for counseling and surveillance of breast cancer patients.
Keywords: breast cancer; lung cancer; radiation exposure; risk ratio.
© 2023 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures
References
-
- Edwards B.K., Noone A.M., Mariotto A.B., Simard E.P., Boscoe F.P., Henley S.J., et al. Annual report to the nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer. 2014;120:1290–1314. - PMC - PubMed
-
- Siegel R.L., Miller K.D., Fuchs H.E., Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7–33. - PubMed
-
- Miller K.D., Nogueira L., Devasia T., Mariotto A.B., Yabroff K.R., Jemal A., et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022;72:409–436. - PubMed
-
- Giuliano A.E., Connolly J.L., Edge S.B., Mittendorf E.A., Rugo H.S., Solin L.J., et al. Breast cancer-major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67:290–303. - PubMed
-
- Amin M.B., Greene F.L., Edge S.B., Compton C.C., Gershenwald J.E., Brookland R.K., et al. The Eighth Edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–99. - PubMed
E-References
-
- Whelan T.J., Pignol J.P., Levine M.N., Julian J.A., MacKenzie R., Parpia S., et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010;362:513–520. - PubMed
-
- Haviland J.S., Owen J.R., Dewar J.A., Agrawal R.K., Barrett J., Barrett-Lee P.J., et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 2013;14:1086–1094. - PubMed
-
- Shah C., Bauer-Nilsen K., McNulty R.H., Vicini F. Novel radiation therapy approaches for breast cancer treatment. Semin Oncol. 2020;47:209–216. - PubMed
-
- Henderson L.M., Rivera M.P., Basch E. Broadened eligibility for lung cancer screening: challenges and uncertainty for implementation and equity. JAMA. 2021;325:939–941. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
