

Alfieri versus conventional repair for bileaflet mitral valve prolapse
- PMID: 38204703
- PMCID: PMC10775110
- DOI: 10.1016/j.xjon.2023.10.005
Alfieri versus conventional repair for bileaflet mitral valve prolapse
Abstract
Objective: Mitral valve repair for bileaflet prolapse can be complex, involving multiple chords or resection. The Alfieri technique for bileaflet disease is simple but may be associated with mitral stenosis or recurrent mitral regurgitation. Outcomes of patients with bileaflet prolapse undergoing mitral valve repair using the Alfieri versus conventional chord/resection techniques were compared.
Methods: Adults undergoing mitral valve repair for bileaflet prolapse for degenerative disease from 2017 to 2023 were stratified by repair technique. Outcomes including operative mortality and echocardiogram data were compared. Time to event analysis was used to characterize freedom from recurrent mitral regurgitation (moderate or greater mitral regurgitation).
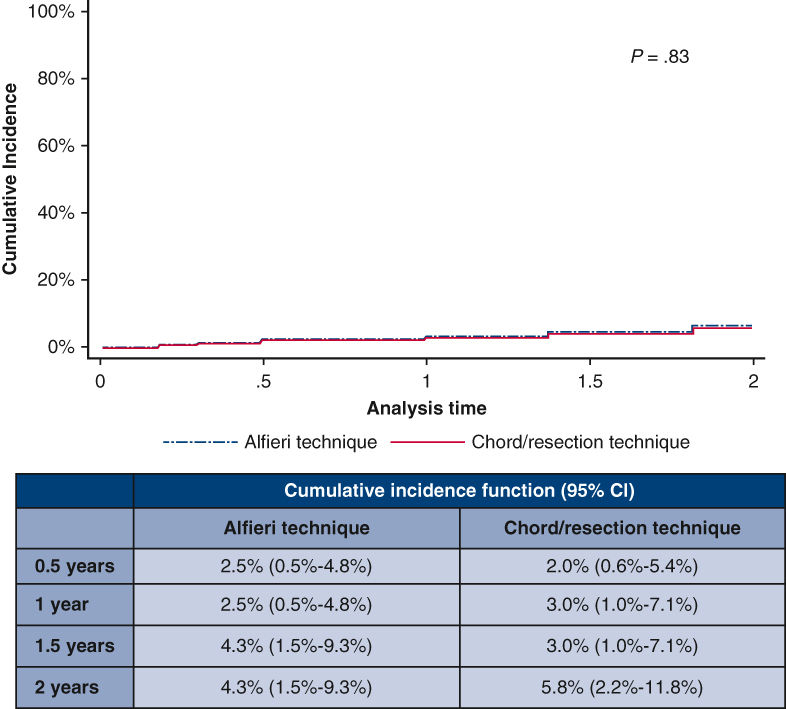
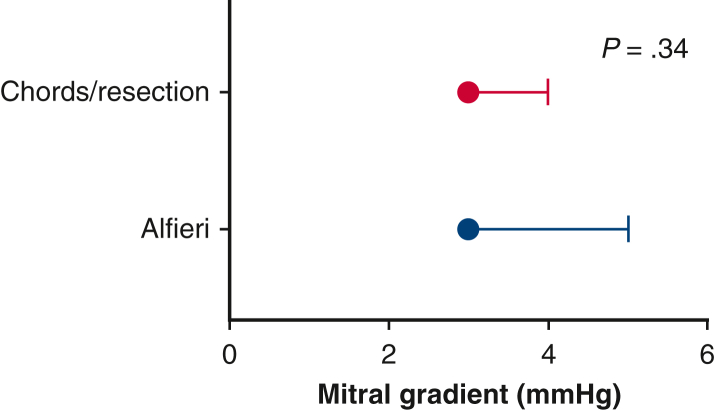
Results: Among 188 patients with bileaflet prolapse, 37% (70) were repaired with the Alfieri and the remaining patients were repaired with chords/resection. Compared with chords/resection, patients undergoing the Alfieri had shorter cardiopulmonary bypass and crossclamp times. Operative mortality (0% [0/70] vs 2% [2/118], P = .27) was similar between both techniques. The mean mitral gradient was low and similar for the Alfieri versus chords/resection (3 vs 3, P = .34). Development of recurrent mitral regurgitation at 2 years, incorporating the competing risk of death and mitral reintervention, was 4.3% (95% CI, 1.5%-9.3%) for the Alfieri technique and 5.8% (95% CI, 2.2%-11.8%) for chord/resection (P = .83).
Conclusions: Both the Alfieri and chord/resection techniques had low rates of recurrent mitral regurgitation at 2 years. The mitral valve gradient was low and similar regardless of technique; thus, those who received the Alfieri technique did not have an increased rate of mitral stenosis. The Alfieri may be an underused technique for bileaflet prolapse.
Keywords: Alfieri; bileaflet prolapse; edge to edge; mitral valve repair.
© 2023 The Author(s).
Conflict of interest statement
G.A. is a consultant for Abbott, Edwards, Medtronic, Anteris, AtriCure, Arthrex, Jena, Ethicon, and Gore. S.F.B. is a consultant for Abbott, Edwards, Medtronic, AtriCure, and Gore. M.A.R. is a consultant for Edwards, Medtronic, and AtriCure. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures





References
-
- da Rocha E Silva J.G., Spampinato R., Misfeld M., Seeburger J., Pfanmüller B., Eifert S., et al. Barlow's mitral valve disease: a comparison of neochordal (loop) and edge-to-edge (Alfieri) minimally invasive repair techniques. Ann Thorac Surg. 2015;100:2127–2133. doi: 10.1016/j.athoracsur.2015.05.097. discussion 2133-5. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
