

Nonelective coronary artery bypass graft outcomes are adversely impacted by Coronavirus disease 2019 infection, but not altered processes of care: A National COVID Cohort Collaborative and National Surgery Quality Improvement Program analysis
- PMID: 38204718
- PMCID: PMC10775046
- DOI: 10.1016/j.xjon.2023.09.020
Nonelective coronary artery bypass graft outcomes are adversely impacted by Coronavirus disease 2019 infection, but not altered processes of care: A National COVID Cohort Collaborative and National Surgery Quality Improvement Program analysis
Abstract
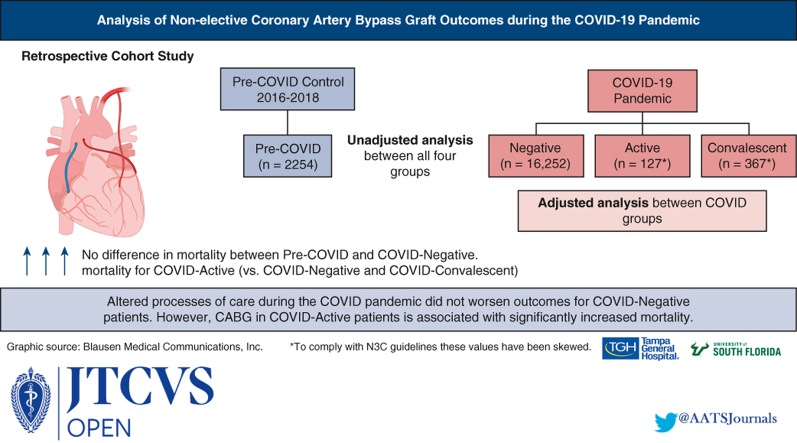
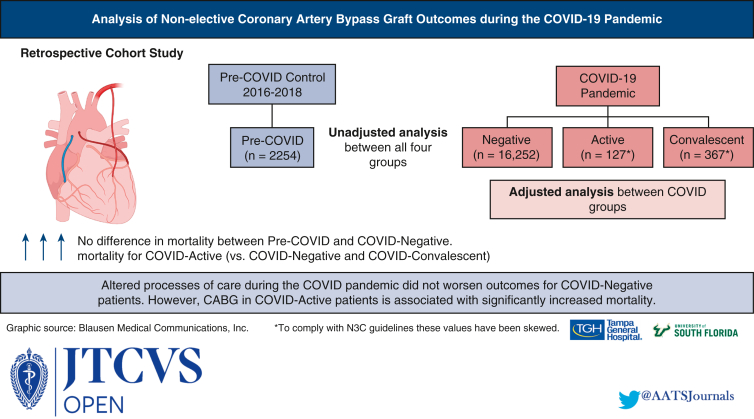
Objective: The effects of Coronavirus disease 2019 (COVID-19) infection and altered processes of care on nonelective coronary artery bypass grafting (CABG) outcomes remain unknown. We hypothesized that patients with COVID-19 infection would have longer hospital lengths of stay and greater mortality compared with COVID-negative patients, but that these outcomes would not differ between COVID-negative and pre-COVID controls.
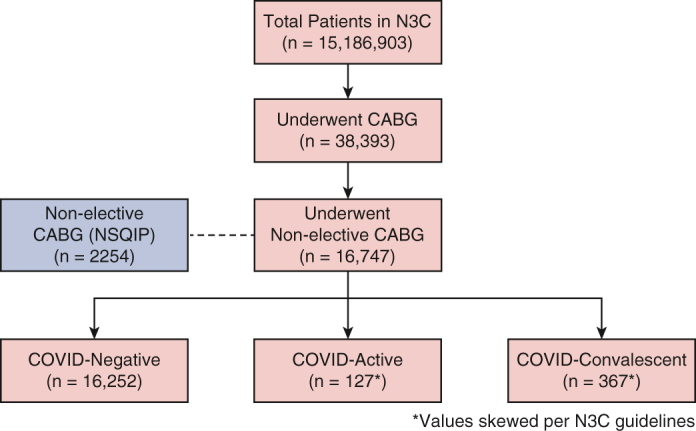
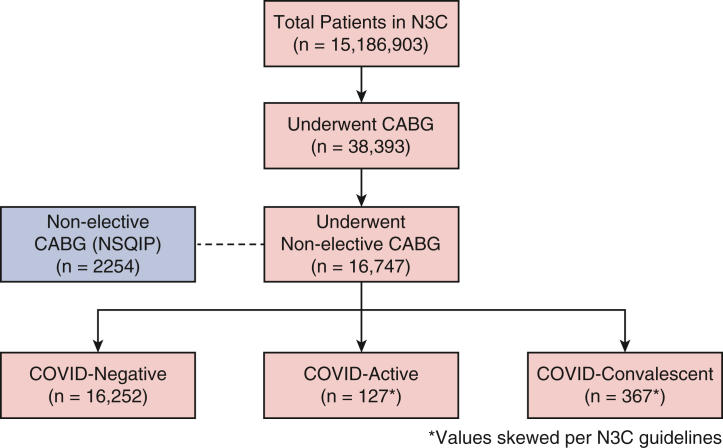
Methods: The National COVID Cohort Collaborative 2020-2022 was queried for adult patients undergoing CABG. Patients were divided into COVID-negative, COVID-active, and COVID-convalescent groups. Pre-COVID control patients were drawn from the National Surgical Quality Improvement Program database. Adjusted analysis of the 3 COVID groups was performed via generalized linear models.
Results: A total of 17,293 patients underwent nonelective CABG, including 16,252 COVID-negative, 127 COVID-active, 367 COVID-convalescent, and 2254 pre-COVID patients. Compared to pre-COVID patients, COVID-negative patients had no difference in mortality, whereas COVID-active patients experienced increased mortality. Mortality and pneumonia were higher in COVID-active patients compared to COVID-negative and COVID-convalescent patients. Adjusted analysis demonstrated that COVID-active patients had higher in-hospital mortality, 30- and 90-day mortality, and pneumonia compared to COVID-negative patients. COVID-convalescent patients had a shorter length of stay but a higher rate of renal impairment.
Conclusions: Traditional care processes were altered during the COVID-19 pandemic. Our data show that nonelective CABG in patients with active COVID-19 is associated with significantly increased rates of mortality and pneumonia. The equivalent mortality in COVID-negative and pre-COVID patients suggests that pandemic-associated changes in processes of care did not impact CABG outcomes. Additional research into optimal timing of CABG after COVID infection is warranted.
Keywords: COVID-19; nonelective coronary artery bypass grafting; outcomes; pandemic.
© 2023 Published by Elsevier Inc. on behalf of The American Association for Thoracic Surgery.
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures
Similar articles
-
Discussion to: Nonelective coronary artery bypass graft outcomes are adversely impacted by Coronavirus disease 2019 infection, but not altered processes of care: A National COVID Cohort Collaborative and National Surgical Quality Improvement Program analysis.JTCVS Open. 2023 Oct 10;16:353-354. doi: 10.1016/j.xjon.2023.10.007. eCollection 2023 Dec. JTCVS Open. 2023. PMID: 38204646 Free PMC article. No abstract available.
-
A cost analysis of nonelective coronary artery bypass graft surgery.J Card Surg. 2006 Nov-Dec;21(6):621-7. doi: 10.1111/j.1540-8191.2006.00315.x. J Card Surg. 2006. PMID: 17073972
-
Coronary artery bypass graft surgery outcomes in the United States: Impact of the coronavirus disease 2019 (COVID-19) pandemic.JTCVS Open. 2021 Jun;6:132-143. doi: 10.1016/j.xjon.2021.03.016. Epub 2021 Mar 30. JTCVS Open. 2021. PMID: 33870234 Free PMC article.
-
Coronary artery bypass grafting in active or recent COVID-19 infection: a systematic review.Indian J Thorac Cardiovasc Surg. 2023 Jul;39(4):350-358. doi: 10.1007/s12055-023-01495-7. Epub 2023 Mar 9. Indian J Thorac Cardiovasc Surg. 2023. PMID: 37342488 Free PMC article. Review.
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
References
Grants and funding
- UL1 TR002649/TR/NCATS NIH HHS/United States
- UL1 TR001433/TR/NCATS NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- UL1 TR001860/TR/NCATS NIH HHS/United States
- UL1 TR001427/TR/NCATS NIH HHS/United States
- U54 GM104942/GM/NIGMS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- UL1 TR001439/TR/NCATS NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
- UL1 TR001445/TR/NCATS NIH HHS/United States
- UL1 TR003096/TR/NCATS NIH HHS/United States
- UM1 TR004556/TR/NCATS NIH HHS/United States
- U54 GM104938/GM/NIGMS NIH HHS/United States
- UL1 TR002537/TR/NCATS NIH HHS/United States
- UL1 TR001412/TR/NCATS NIH HHS/United States
- UL1 TR001872/TR/NCATS NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- UL1 TR002529/TR/NCATS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UL1 TR002494/TR/NCATS NIH HHS/United States
- UL1 TR002736/TR/NCATS NIH HHS/United States
- U54 GM115516/GM/NIGMS NIH HHS/United States
- UL1 TR002369/TR/NCATS NIH HHS/United States
- UL1 TR002541/TR/NCATS NIH HHS/United States
- U54 GM115371/GM/NIGMS NIH HHS/United States
- UL1 TR002001/TR/NCATS NIH HHS/United States
- UL1 TR002538/TR/NCATS NIH HHS/United States
- U54 GM115458/GM/NIGMS NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- UL1 TR002535/TR/NCATS NIH HHS/United States
- UL1 TR001866/TR/NCATS NIH HHS/United States
- UL1 TR003167/TR/NCATS NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- UL1 TR001453/TR/NCATS NIH HHS/United States
- UL1 TR002489/TR/NCATS NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- UL1 TR003107/TR/NCATS NIH HHS/United States
- UL1 TR003015/TR/NCATS NIH HHS/United States
- UL1 TR002733/TR/NCATS NIH HHS/United States
- U24 TR002306/TR/NCATS NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
- UL1 TR001876/TR/NCATS NIH HHS/United States
- UL1 TR001436/TR/NCATS NIH HHS/United States
- UL1 TR002378/TR/NCATS NIH HHS/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- UL1 TR002553/TR/NCATS NIH HHS/United States
- UL1 TR002389/TR/NCATS NIH HHS/United States
- UL1 TR001414/TR/NCATS NIH HHS/United States
- U54 GM104941/GM/NIGMS NIH HHS/United States
- UL1 TR002014/TR/NCATS NIH HHS/United States
- UL1 TR002550/TR/NCATS NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- UL1 TR001855/TR/NCATS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- UL1 TR002373/TR/NCATS NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- UL1 TR002556/TR/NCATS NIH HHS/United States
- UL1 TR003017/TR/NCATS NIH HHS/United States
- UL1 TR001998/TR/NCATS NIH HHS/United States
- UL1 TR001873/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UL1 TR002645/TR/NCATS NIH HHS/United States
- UL1 TR001450/TR/NCATS NIH HHS/United States
- UL1 TR002366/TR/NCATS NIH HHS/United States
- U54 GM115428/GM/NIGMS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- UL1 TR002377/TR/NCATS NIH HHS/United States
- U54 GM115677/GM/NIGMS NIH HHS/United States
- UL1 TR002544/TR/NCATS NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- UL1 TR001430/TR/NCATS NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
