

Cancer-Associated Thrombosis: Trends in Clinical Features, Treatment, and Outcomes From 2001 to 2020
- PMID: 38205016
- PMCID: PMC10774792
- DOI: 10.1016/j.jaccao.2023.09.003
Cancer-Associated Thrombosis: Trends in Clinical Features, Treatment, and Outcomes From 2001 to 2020
Abstract
Background: Despite advances in cancer and venous thromboembolism (VTE) management, the epidemiology of cancer-associated thrombosis management over time remains unclear.
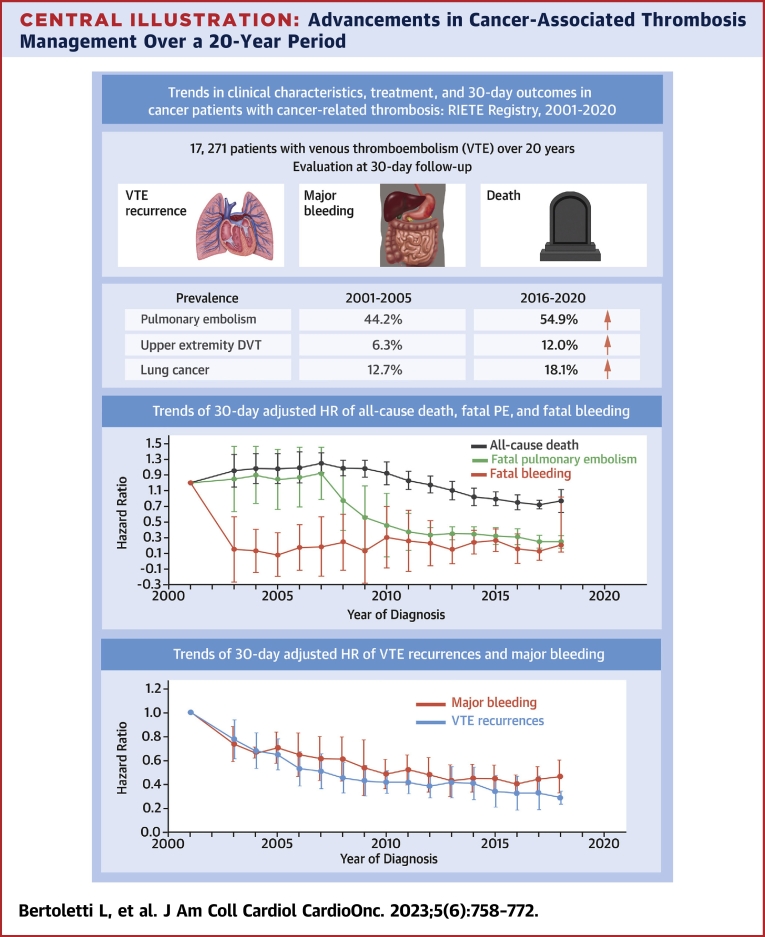
Objectives: We analyzed data from the RIETE (Registro Informatizado de la Enfermedad Trombo Embólica) registry spanning 2001 to 2020 to investigate temporal trends in clinical characteristics and treatments for cancer-associated thrombosis.
Methods: Using multivariable survival regression, we examined temporal trends in risk-adjusted rates of symptomatic VTE recurrences, major bleeding, and death within 30 days after incident VTE.
Results: Among the 17,271 patients with cancer-associated thrombosis, there was a progressive increase in patients presenting with pulmonary embolism (from 44% in 2001-2005 to 55% in 2016-2020; P < 0.001 for trend), lung (from 12.7% to 18.1%; P < 0.001) or pancreatic cancer (from 3.8% to 5.6%; P = 0.003), and utilization of immunotherapy (from 0% to 7.4%; P < 0.001). Conversely, there was a decline in patients with prostate cancer (from 11.7% to 6.6%; P < 0.001) or carcinoma of unknown origin (from 3.5% to 0.7%; P < 0.001). At the 30-day follow-up, a reduction was observed in the proportion of patients experiencing symptomatic VTE recurrences (from 3.1% to 1.1%; P < 0.001), major bleeding (from 3.1% to 2.2%; P = 0.004), and death (from 11.9% to 8.4%; P < 0.001). Multivariable analyses revealed a decreased risk over time for VTE recurrence (adjusted subdistribution HR [asHR]: 0.94 per year; 95% CI: 0.92-0.98), major bleeding (asHR: 0.98; 95% CI: 0.96-0.99), and death (aHR: 0.97; 95% CI: 0.96-0.98).
Conclusions: In this multicenter study of cancer patients with VTE, there was a decline in thrombotic, hemorrhagic, and fatal events from 2001 to 2020. (Registro Informatizado de la Enfermedad Trombo Embólica [RIETE]; NCT02832245).
Keywords: anticoagulant; bleeding; cancer; survival; thrombosis.
© 2023 The Authors.
Conflict of interest statement
Dr Bertoletti has received personal fees and nonfinancial support from Aspen, Bayer, BMS-Pfizer, and Léo-Pharma and Johnson & Johnson; and has received grants, personal fees, and nonfinancial support from Merck Sharp & Dohme outside the submitted work. Dr Jimenez has received grants or contracts from Daiichi-Sankyo, Sanofi, and ROVI; and has received personal fees and honoraria for lectures from Bayer, Boehringer Ingelheim, BMS, Daiichi-Sankyo, Léo-Pharma, Pfizer, ROVI, and Sanofi outside the submitted work. Dr Bikdeli is supported by the Scott Schoen and Nancy Adams IGNITE Award from the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and a Career Development Award from the American Heart Association (#938814). Dr Ay has received honoraria for lectures from Bayer, BMS, Daiichi-Sankyo, Pfizer, and Sanofi outside the submitted work; and has served on Advisory Boards of Bayer, BMS, Daiichi-Sankyo, Pfizer, and Sanofi. Dr Trujillo-Santos has received personal fees and honoraria for lectures from Bayer, Boehringer Ingelheim, BMS, Daiichi-Sankyo, Léo-Pharma, Pfizer, ROVI, and Sanofi outside the submitted work. Dr Sigüenza has received support for attending meetings for Sanofi, ROVI, and Viatris. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures







References
-
- Grilz E., Posch F., Nopp S., et al. Relative risk of arterial and venous thromboembolism in persons with cancer vs. persons without cancer-a nationwide analysis. Eur Heart J. 2021;42(23):2299–2307. - PubMed
-
- Ay C., Pabinger I., Cohen A.T. Cancer-associated venous thromboembolism: burden, mechanisms, and management. Thromb Haemost. 2017;117(2):219–230. - PubMed
-
- Mulder F.I., Horváth-Puhó E., van Es N., et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021;137(14):1959–1969. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
