

Comparative before-after study of fever prevention versus targeted temperature management following out-of-hospital cardiac arrest
- PMID: 38205148
- PMCID: PMC10776978
- DOI: 10.1016/j.resplu.2023.100538
Comparative before-after study of fever prevention versus targeted temperature management following out-of-hospital cardiac arrest
Abstract
Background: International guidelines for neuroprotection following out-of-hospital cardiac arrest (OHCA) recommend fever prevention ahead of routine temperature management. This study aimed to identify any effect of changing from targeted temperature management to fever prevention on neurological outcome following OHCA.
Methods: A retrospective observational cohort study was conducted of consecutive admissions to an ICU at a tertiary OHCA centre. Comparison was made between a period of protocolised targeted temperature management (TTM) to 36 °C and a period of fever prevention.
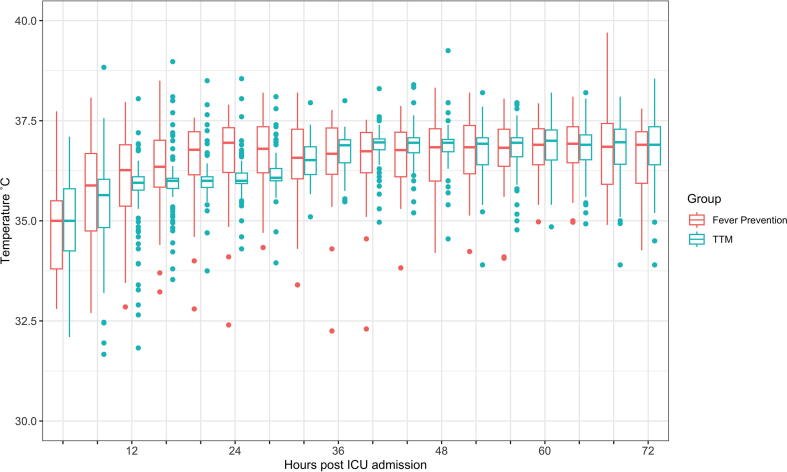
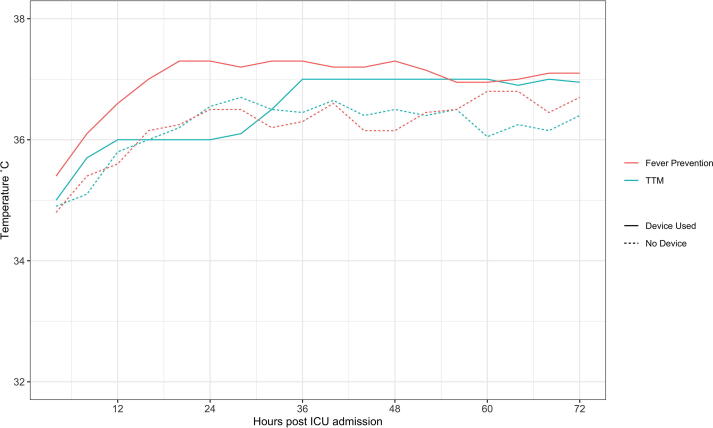
Results: Data were available for 183 patients. Active temperature management was administered in 86/118 (72%) of the TTM cohort and 20/65 (31%) of the fever prevention group. The median highest temperature prior to the start of temperature management was significantly lower in the TTM group at 35.6 (IQR 34.9-36.2) compared to 37.9 °C (IQR 37.7-38.2) in the fever prevention group (adjusted p < 0.001).There was no difference in the proportion of patients discharged with Cerebral Performance Category 1 or 2 between the groups (42% vs. 40%, p = 0.88). Patients in the fever prevention group required a reduced duration of noradrenaline (36 vs. 46 h, p = 0.03) and a trend towards a reduced duration of propofol (37 vs. 56 h, p = 0.06).In unadjusted analysis, use of active temperature management (irrespective of group) appeared to be associated with decreased risk of poor outcome (OR = 0.43, 95% CI 0.23-0.78) but after adjustment for patient age, presenting rhythm, witnessed arrest and duration of CPR, this was no longer significant (OR = 0.93, 95% CI 0.37-2.31, p = 0.88).
Conclusion: Switching from TTM to fever prevention following OHCA was associated with similar rates of neurological outcomes, with a possible decrease in sedation and vasopressor requirements.
Keywords: Neuroprognostication; Out-of-Hospital Cardiac Arrest; Targeted temperature management; Therapeutic Hypothermia.
© 2023 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: [AP is funded by a Medical Research Council Clinical Academic Research Partnership Award (Ref:MR/W03011X/1) and the Barts Charity. All other authors declare no conflict of interest.].
Figures
References
-
- Zeiner A., Holzer M., Sterz F., et al. Hyperthermia after cardiac arrest is associated with an unfavorable neurologic outcome. Arch Intern Med. 2001;161:2007. - PubMed
-
- Nielsen N., Wetterslev J., Cronberg T., et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369:2197–2206. - PubMed
-
- Dankiewicz J., Cronberg T., Lilja G., et al. Hypothermia versus normothermia after out-of-hospital cardiac arrest. N Engl J Med. 2021;384:2283–2294. - PubMed
-
- Hypothermia after Cardiac Arrest Study Group. Mild Therapeutic Hypothermia to Improve the Neurologic Outcome after Cardiac Arrest. N Engl J Med. 2002;346:549–56. - PubMed
-
- Bernard S.A., Gray T.W., Buist M.D., et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
