

Sodium and Its Impact on Outcome After Aneurysmal Subarachnoid Hemorrhage in Patients With and Without Delayed Cerebral Ischemia
- PMID: 38206089
- PMCID: PMC11008454
- DOI: 10.1097/CCM.0000000000006182
Sodium and Its Impact on Outcome After Aneurysmal Subarachnoid Hemorrhage in Patients With and Without Delayed Cerebral Ischemia
Abstract
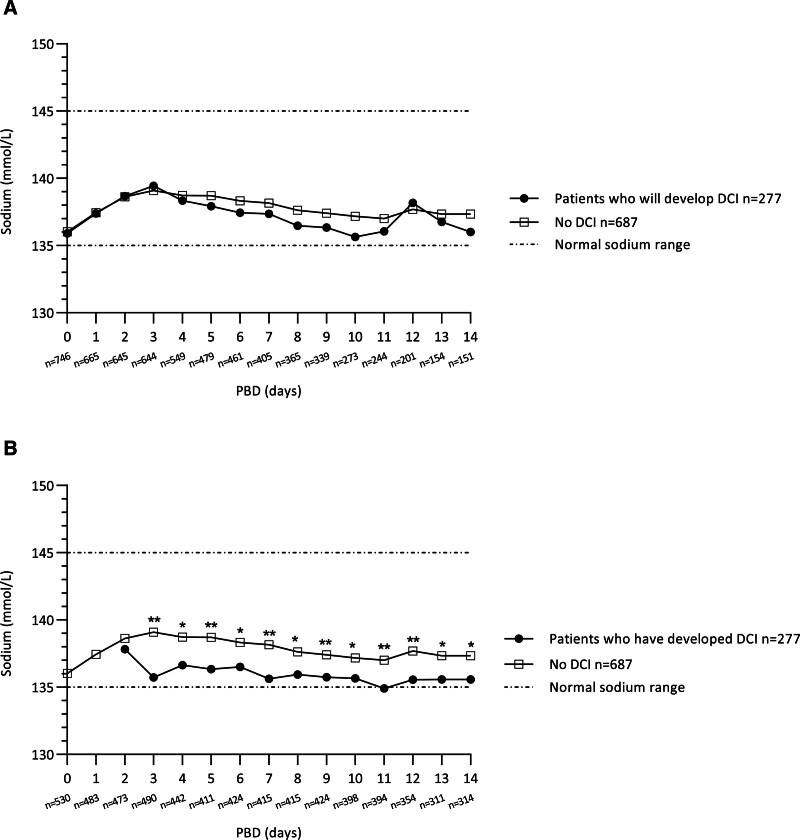
Objectives: To perform a detailed examination of sodium levels, hyponatremia and sodium fluctuations, and their association with delayed cerebral ischemia (DCI) and poor outcome after aneurysmal subarachnoid hemorrhage (aSAH).
Design: An observational cohort study from a prospective SAH Registry.
Setting: Tertiary referral center focused on SAH treatment in the Amsterdam metropolitan area.
Patients: A total of 964 adult patients with confirmed aSAH were included between 2011 and 2021.
Interventions: None.
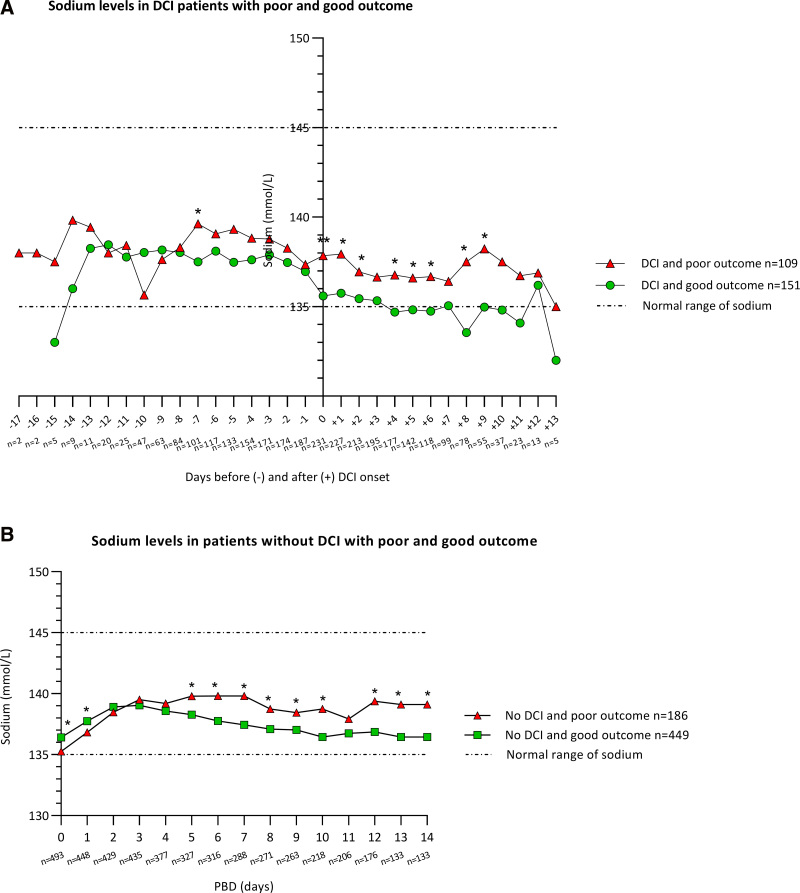
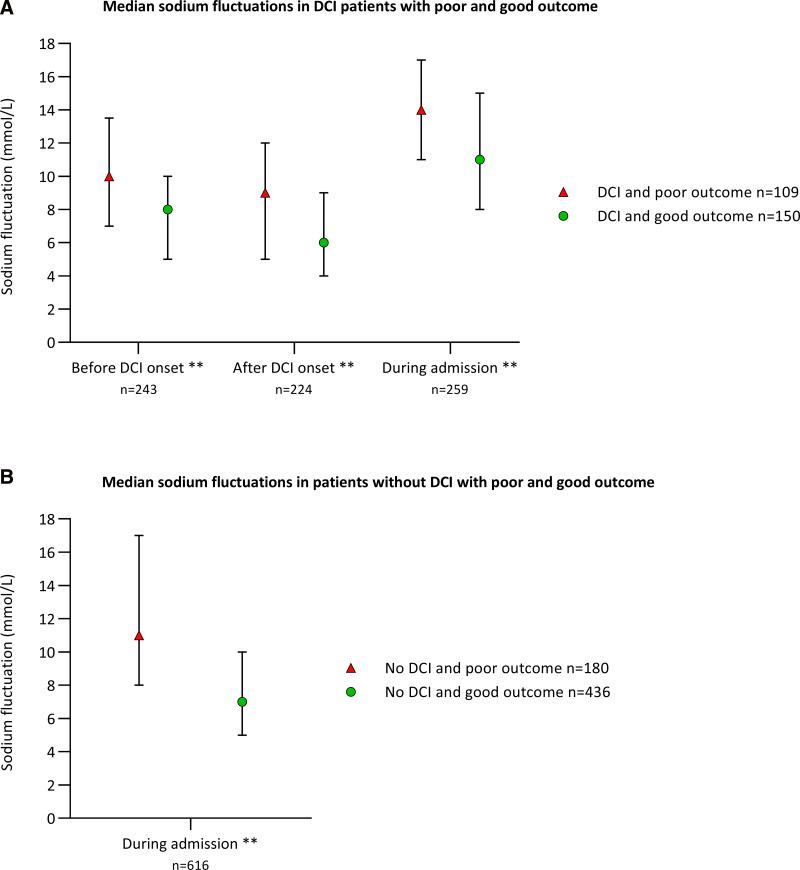
Measurements and main results: A total of 277 (29%) developed DCI. Hyponatremia occurred significantly more often in DCI patients compared with no-DCI patients (77% vs. 48%). Sodium levels, hyponatremia, hypernatremia, and sodium fluctuations did not predict DCI. However, higher sodium levels were significantly associated with poor outcome in DCI patients (DCI onset -7, DCI +0, +1, +2, +4, +5, +8, +9 d), and in no-DCI patients (postbleed day 6-10 and 12-14). Also, hypernatremia and greater sodium fluctuations were significantly associated with poor outcome in both DCI and no-DCI patients.
Conclusions: Sodium levels, hyponatremia, and sodium fluctuations were not associated with the occurrence of DCI. However, higher sodium levels, hypernatremia, and greater sodium fluctuations were associated with poor outcome after aSAH irrespective of the presence of DCI. Therefore, sodium levels, even with mild changes in levels, warrant close attention.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Labib disclosed work for hire. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- van Gijn J, Kerr RS, Rinkel GJE: Subarachnoid haemorrhage. Lancet. 2007; 369:306–318 - PubMed
-
- Feigin VL, Lawes CM, Bennett DA, et al. : Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 2009; 8:355–369 - PubMed
-
- Nieuwkamp DJ, Setz LE, Algra A, et al. : Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: A meta-analysis. Lancet Neurol. 2009; 8:635–642 - PubMed
-
- Al-Khindi T, MacDonald RL, Schweizer TA: Cognitive and functional outcome after aneurysmal subarachnoid hemorrhage. Stroke. 2010; 41:e519–e536 - PubMed
-
- Duan W, Pan Y, Wang C, et al. : Risk factors and clinical impact of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: Analysis from the China National Stroke Registry. Neuroepidemiology. 2018; 50:128–136 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
