

A proposed index of myocardial staining for vein of Marshall ethanol infusion: an Italian single-center experience
- PMID: 38206450
- PMCID: PMC11288988
- DOI: 10.1007/s10840-023-01732-4
A proposed index of myocardial staining for vein of Marshall ethanol infusion: an Italian single-center experience
Abstract
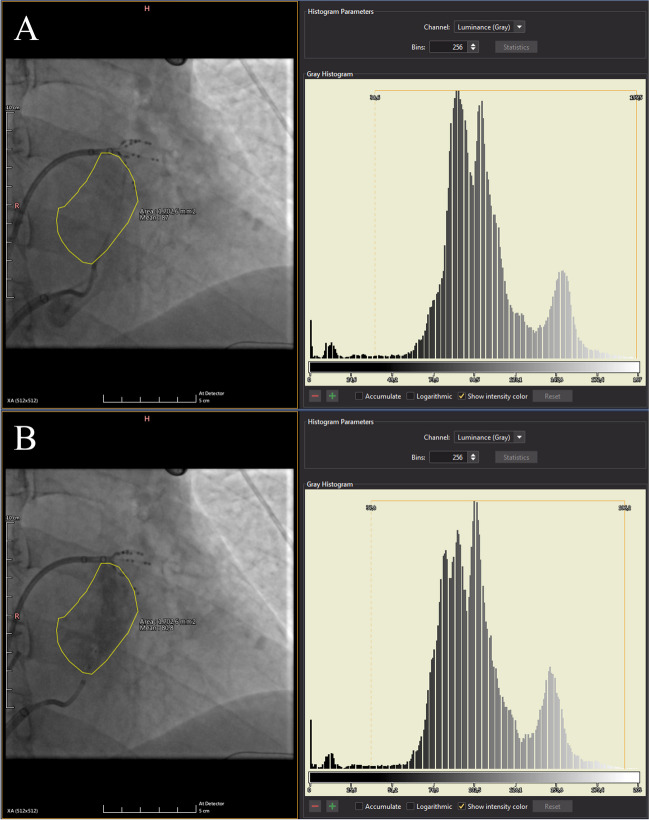
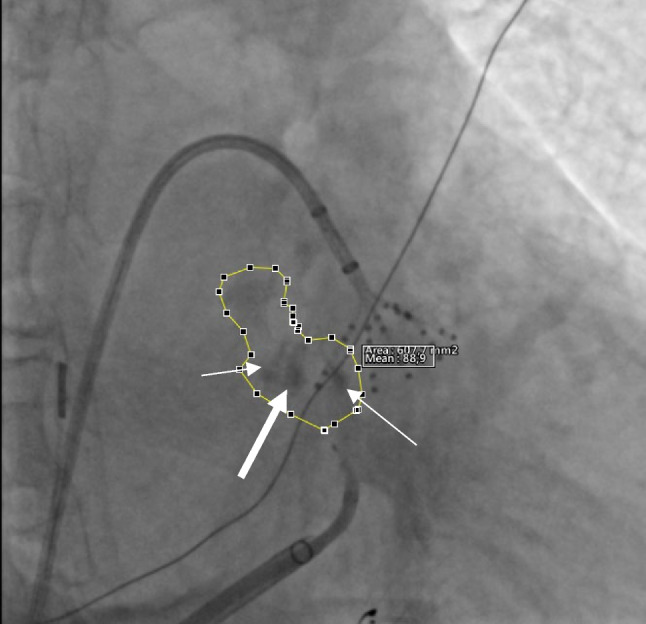
Background: Mitral isthmus (MI) conduction block is a fundamental step in anatomical approach treatment for persistent atrial fibrillation (PeAF). However, MI block is hardly achievable with endocardial ablation only. Retrograde ethanol infusion (EI) into the vein of Marshall (VOM) facilitates MI block. Fluorographic myocardial staining (MS) during VOM-EI could be helpful in predicting procedural alcoholization outcome even if its role is qualitatively assessed in the routine. The aim was to quantitatively assess MS during VOM-EI and to evaluate its association with MI block achievement.
Methods: Consecutive patients undergoing catheter ablation for PeAF at Fondazione Toscana Gabriele Monasterio (Pisa, Italy) from February 2022 to May 2023 were considered. Patients with identifiable VOM were included. A proposed index of MS (MSI) was retrospectively calculated in each included patient. Correlation of MSI with low-voltage zones (LVZ) extension after VOM-EI and its association with MI block achievement were assessed.
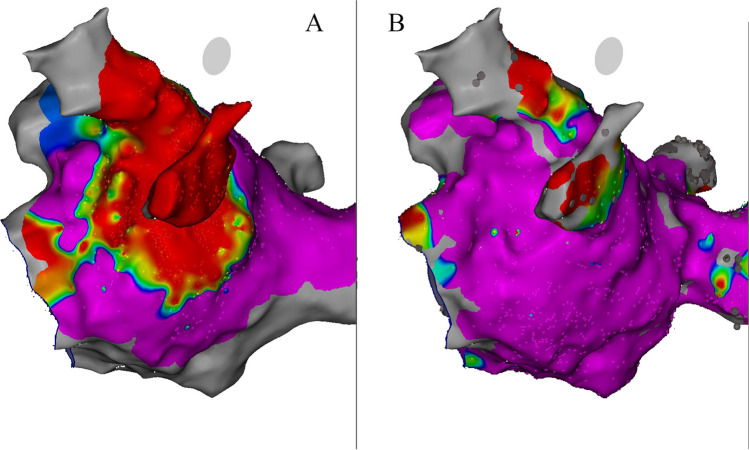
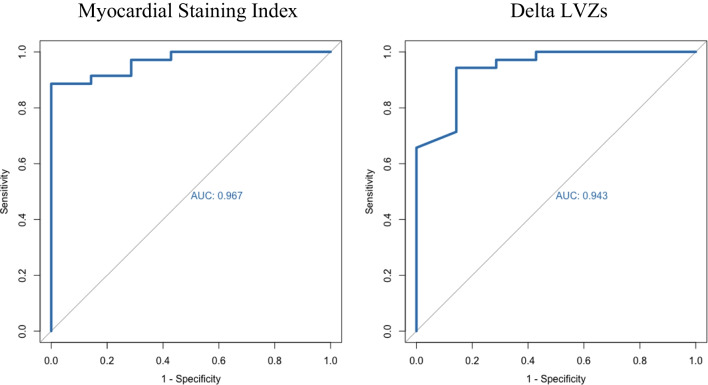
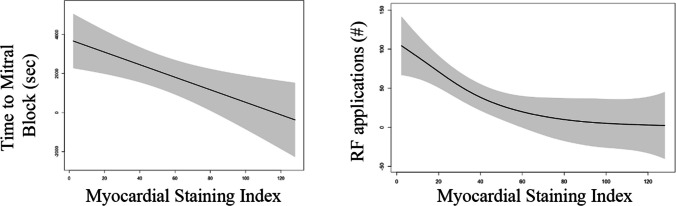
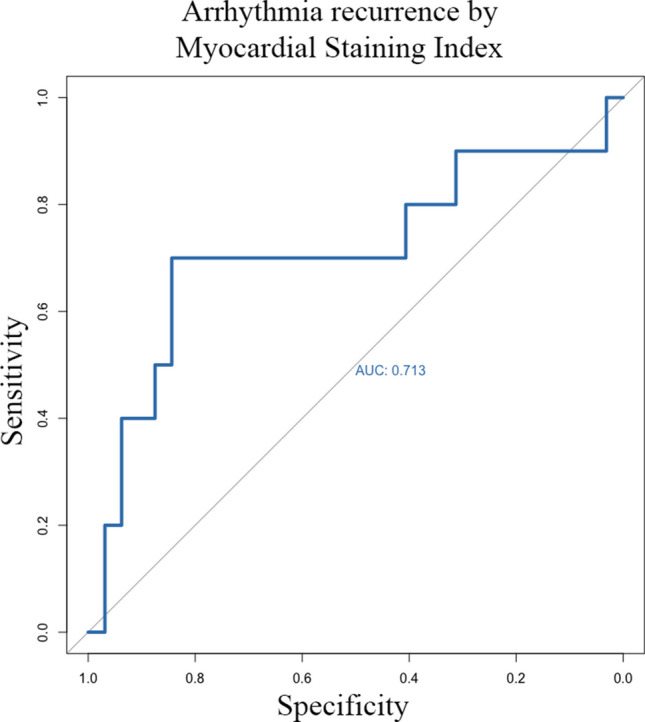
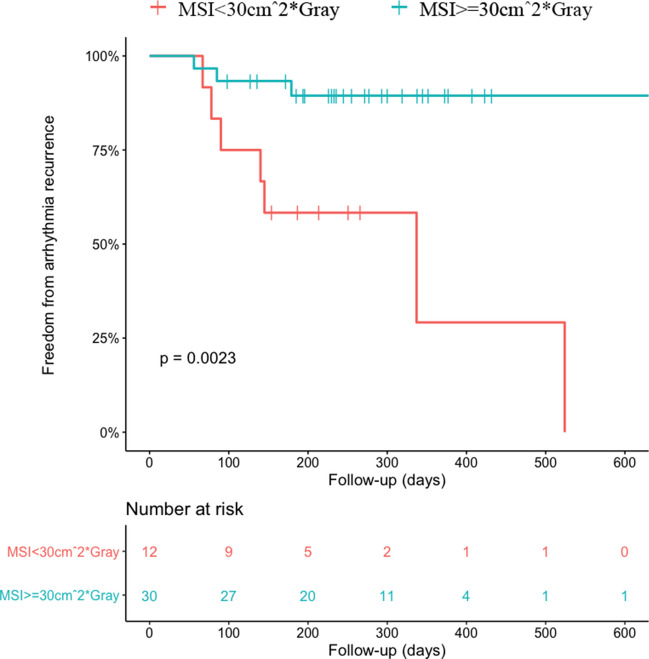
Results: In total, 42 patients out of 49 (85.8%) had an identifiable VOM. MI block was successfully achieved in 35 patients out of 42 (83.3%). MSI was significantly associated with the occurrence of MI block (OR 1.24 (1.03-1.48); p = 0.022). A higher MSI resulted in reduced ablation time (p = 0.014) and reduced radiofrequency applications (p = 0.002) to obtain MI block. MSI was also associated with MI block obtained by endocardial ablation only (OR 1.07 (1.02-1.13); p = 0.002). MSI was highly correlated with newly formed LVZ extension (r = 0.776; p = 0.001).
Conclusions: In our study cohort, optimal MSI predicts MI block and facilitates its achievement with endocardial ablation only.
Keywords: Catheter ablation; Ethanol infusion; Mitral isthmus; Persistent atrial fibrillation; Staining; Vein of Marshall.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Verma A, Jian C, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812–22. - PubMed
-
- Pambrun T, Derval N, Duchateau J, Denis A, Chauvel R, Tixier R, et al. Epicardial course of the musculature related to the great cardiac vein: anatomical considerations and clinical implications for mitral isthmus block after vein of Marshall ethanol infusion. Heart Rhythm. 2021;18(11):1951–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
