

Uterine injury during diestrus leads to placental and embryonic defects in future pregnancies in mice†
- PMID: 38206869
- PMCID: PMC11017118
- DOI: 10.1093/biolre/ioae001
Uterine injury during diestrus leads to placental and embryonic defects in future pregnancies in mice†
Abstract
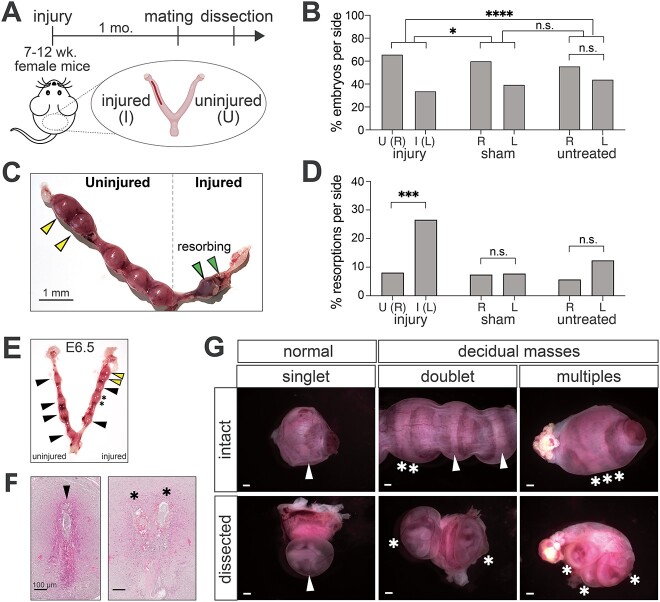
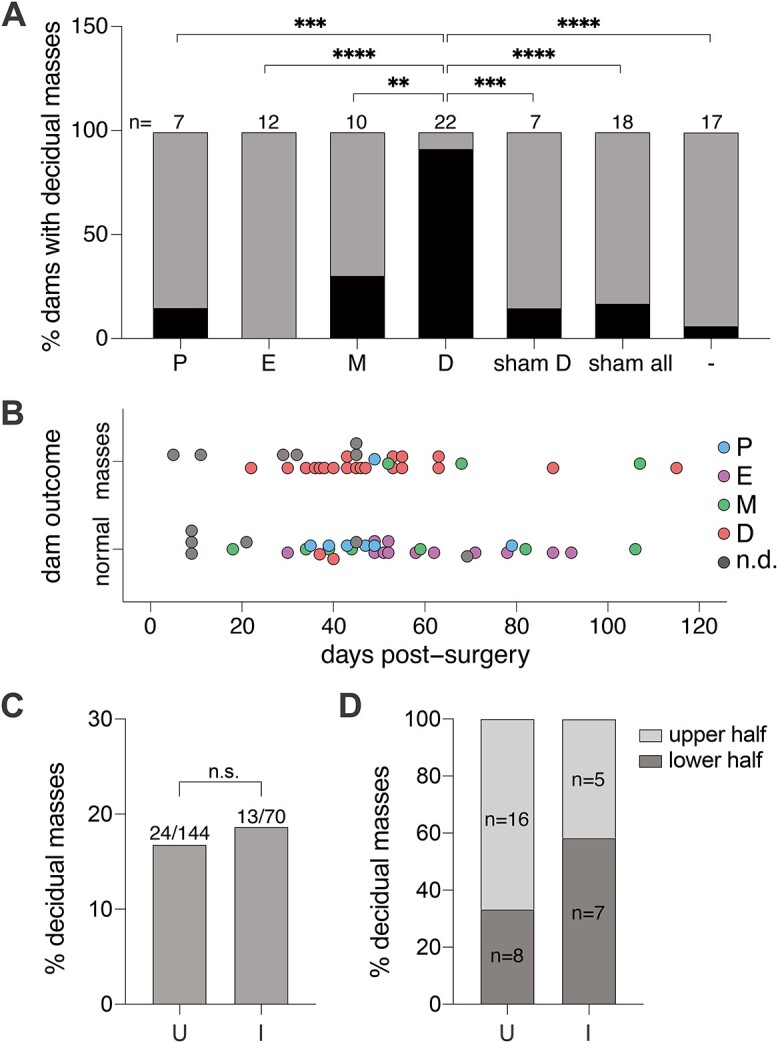
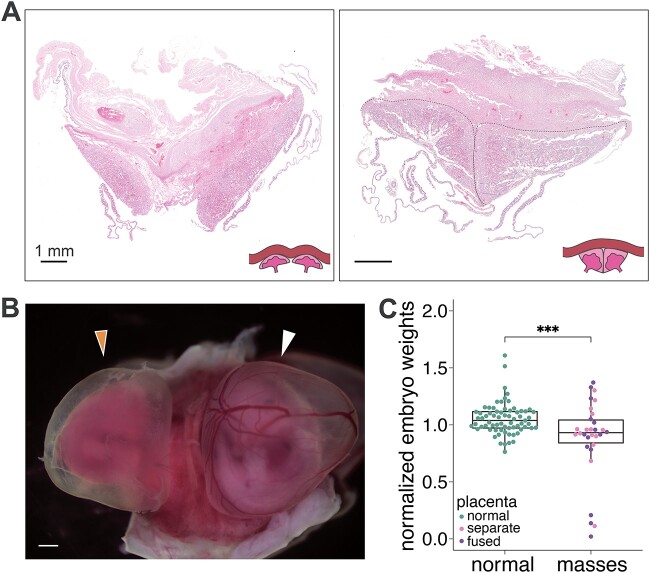
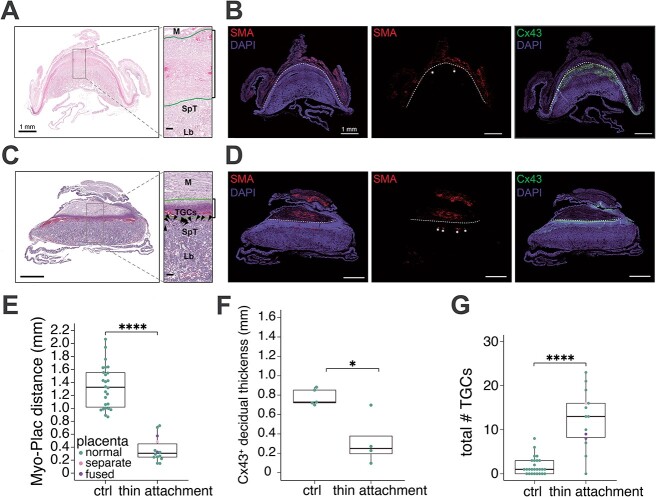
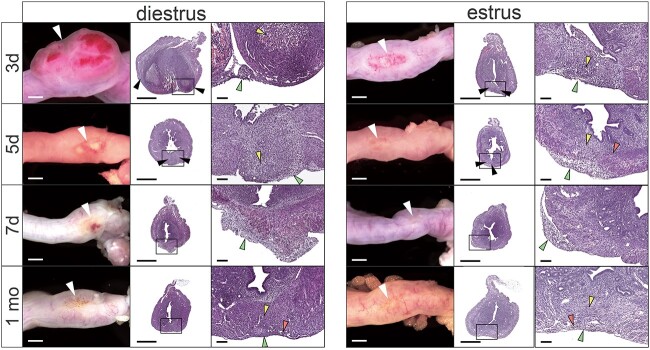
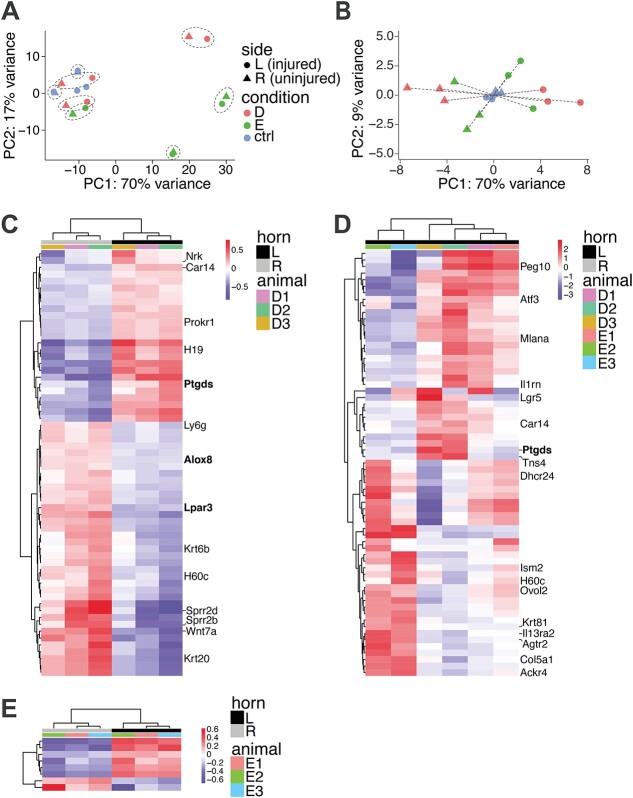
Uterine injury from procedures such as Cesarean sections (C-sections) often have severe consequences on subsequent pregnancy outcomes, leading to disorders such as placenta previa, placenta accreta, and infertility. With rates of C-section at ~30% of deliveries in the USA and projected to continue to climb, a deeper understanding of the mechanisms by which these pregnancy disorders arise and opportunities for intervention are needed. Here we describe a rodent model of uterine injury on subsequent in utero outcomes. We observed three distinct phenotypes: increased rates of resorption and death, embryo spacing defects, and placenta accreta-like features of reduced decidua and expansion of invasive trophoblasts. We show that the appearance of embryo spacing defects depends entirely on the phase of estrous cycle at the time of injury. Using RNA-seq, we identified perturbations in the expression of components of the COX/prostaglandin pathway after recovery from injury, a pathway that has previously been demonstrated to play an important role in embryo spacing. Therefore, we demonstrate that uterine damage in this mouse model causes morphological and molecular changes that ultimately lead to placental and embryonic developmental defects.
Keywords: C-section; embryo spacing; injury; placenta accreta; placenta previa; pregnancy; uterus; wound healing.
© The Author(s) 2024. Published by Oxford University Press on behalf of Society for the Study of Reproduction. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Wortman AC, Alexander JM. Placenta accreta, increta, and percreta. Obstet Gynecol Clin North Am 2013; 40:137–154. - PubMed
-
- Silver RM, Barbour KD. Placenta accreta spectrum: accreta, increta, and percreta. Obstet Gynecol Clin North Am 2015; 42:381–402. - PubMed
-
- Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: twenty-year analysis. Am J Obstet Gynecol 2005; 192:1458–1461. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
