

Overuse of computed tomography for mild head injury: A systematic review and meta-analysis
- PMID: 38206917
- PMCID: PMC10783716
- DOI: 10.1371/journal.pone.0293558
Overuse of computed tomography for mild head injury: A systematic review and meta-analysis
Abstract
Background: Computed tomography (CT) scan is a common imaging technique used to evaluate the severity of a head injury. The overuse of diagnostic interventions in the health system is a growing concern worldwide. Objectives: The aim of this systematic review is to investigate the rate of CT scan overuse in cases of mild head injury.
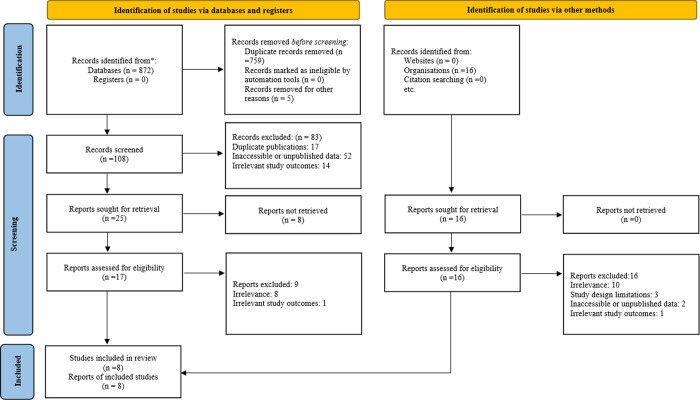
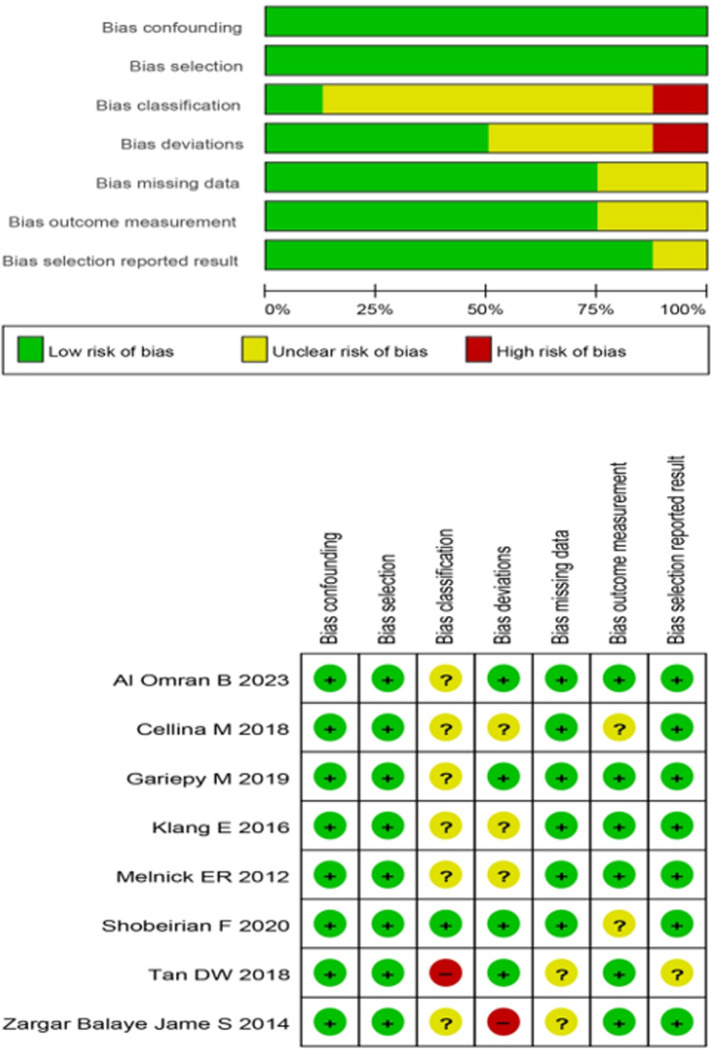
Methods: Eligibility criteria: We encompassed observational studies-either designed as cohort, case-control, or cross-sectional investigations-that reported on CT scan overuse rates for mild head injuries. Studies had to be published in peer-reviewed, English-language sources and provide full content access Information sources: Web of Sciences, Scopus, Medline via PubMed, the Cochrane Library and Embase were searched from inception until April 1, 2023. Studies were included if reporting the overuse of CT scans for mild head injuries using validated criteria. Risk of bias: We used the Risk Of Bias In Non-randomised Studies - of Interventions (ROBINS-I) tool to evaluate the risk bias assessment of included studies. Two independent reviewers evaluated the eligibility of studies, extracted data, and assessed study quality by using the Newcastle-Ottawa Scale. Synthesis of results: Overuse estimates were calculated using a random-effects model. Subgroup analyses were performed to investigate any sources of heterogeneity. Point rate of overuse of CT scans for mild head injuries was the main outcome measured as percentage point estimates with corresponding 95% CIs.
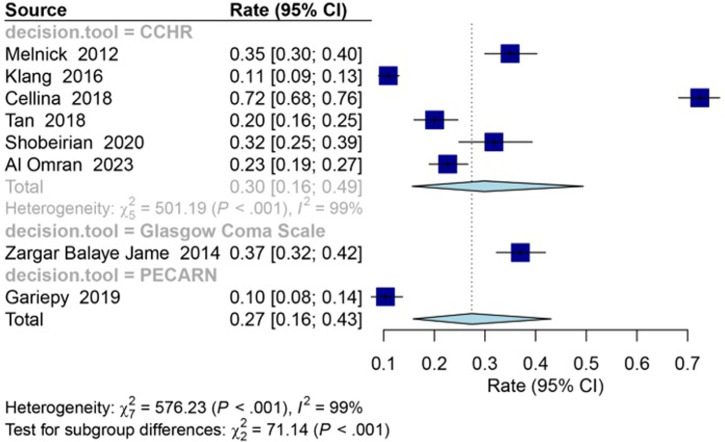
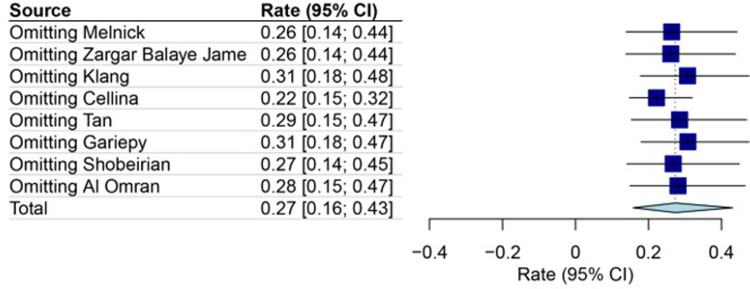
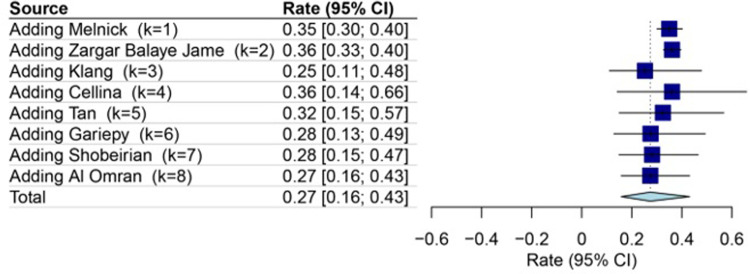
Results: Included studies: Of the 913 potentially relevant studies identified, eight studies were selected for the final analysis. Synthesis of results: The pooled rate of CT scan overuse in patients with mild head injury was found to be 27% [95% CI: 16-43; I2 = 99%]. The rate of CT scan overuse in mild head injury cases varied depending on the criteria used. The rate of CT scan overuse was 37% [95% CI: 32-42; I2 = 0%] with the Glasgow Coma Scale (GCS), 30% [95% CI: 16-49; I2 = 99%] with the Canadian computed tomography head rule, and 10% [95% CI: 8-14; I2 = 0%] with the Pediatric Emergency Care Applied Research Network criterion (PERCAN). Based on subgroup analyses, the rate of CT scan overuse in mild head injury cases was observed to be 30% with the Canadian computed tomography head rule criterion, 43% with the National Institute for Health and Clinical Excellence criterion, and 18% with the New Orleans criterion.
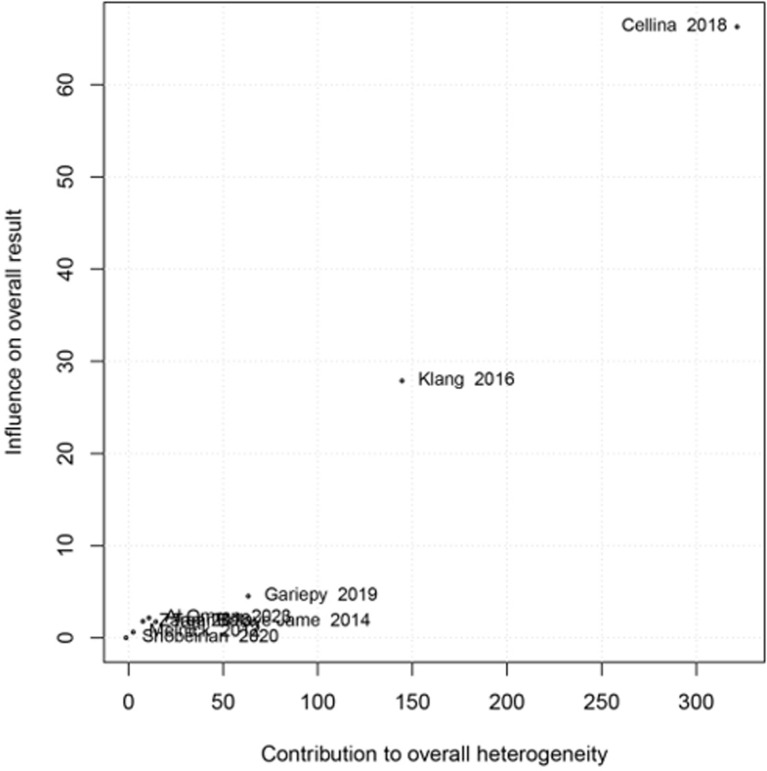
Conclusion: Limitations of evidence: The restricted number of included studies may impact generalizability. High heterogeneity was observed, leading to subgroup analyses based on age, assessment criteria, and study region. Absent data on overuse causes hinders drawing conclusions on contributing factors. Furthermore, this study solely addressed overuse rates, not associated harm or benefits. Interpretation: The overuse of CT scans in mild head injury patients is concerning, as it can result in unnecessary radiation exposure and higher healthcare costs. Clinicians and policymakers should prioritize the implementation of guidelines to reduce unnecessary radiation exposure, healthcare costs, and potential harm to patients.
Trial registration: The study protocol of this review was registered in PROSPERO under the identification code CRD42023416080. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023416080.
Copyright: © 2024 Saran et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Risk factors for traumatic intracranial hemorrhage in mild traumatic brain injury patients at the emergency department: a systematic review and meta-analysis.Scand J Trauma Resusc Emerg Med. 2024 Sep 17;32(1):91. doi: 10.1186/s13049-024-01262-6. Scand J Trauma Resusc Emerg Med. 2024. PMID: 39289729 Free PMC article.
-
Prediction value of the Canadian CT head rule and the New Orleans criteria for positive head CT scan and acute neurosurgical procedures in minor head trauma: a multicenter external validation study.Ann Emerg Med. 2013 May;61(5):521-7. doi: 10.1016/j.annemergmed.2012.07.016. Epub 2012 Aug 22. Ann Emerg Med. 2013. PMID: 22921164
-
Overuse of computed tomography for minor head injury in young patients: an analysis of promoting factors.Radiol Med. 2018 Jul;123(7):507-514. doi: 10.1007/s11547-018-0871-x. Epub 2018 Mar 7. Radiol Med. 2018. PMID: 29516354
-
Accuracy of Canadian CT head rule in predicting positive findings on CT of the head of patients after mild head injury in a large trauma centre in Saudi Arabia.Neuroradiol J. 2015 Dec;28(6):591-7. doi: 10.1177/1971400915610699. Epub 2015 Oct 15. Neuroradiol J. 2015. PMID: 26471399 Free PMC article.
-
Effectiveness of implementation strategies for increasing clinicians' use of five validated imaging decision rules for musculoskeletal injuries: a systematic review.BMC Emerg Med. 2024 May 17;24(1):84. doi: 10.1186/s12873-024-00996-x. BMC Emerg Med. 2024. PMID: 38760697 Free PMC article.
Cited by
-
Risk factors for traumatic intracranial hemorrhage in mild traumatic brain injury patients at the emergency department: a systematic review and meta-analysis.Scand J Trauma Resusc Emerg Med. 2024 Sep 17;32(1):91. doi: 10.1186/s13049-024-01262-6. Scand J Trauma Resusc Emerg Med. 2024. PMID: 39289729 Free PMC article.
-
Overuse of medical imaging and effects of payer-provider integration: quasi-experimental evidence from Finland.Health Econ Rev. 2025 Jan 28;15(1):4. doi: 10.1186/s13561-025-00592-0. Health Econ Rev. 2025. PMID: 39873926 Free PMC article.
-
Analysis of Cases of Mild Head Trauma Resulting in Fatal Outcome from the Doctor Helicopter Registry Data.J Emerg Trauma Shock. 2025 Apr-Jun;18(2):53-55. doi: 10.4103/jets.jets_87_24. Epub 2025 Jun 19. J Emerg Trauma Shock. 2025. PMID: 40666395 Free PMC article.
-
Trends in CT use in an emergency department in Western Australia: 2015-2022.Insights Imaging. 2025 Jun 4;16(1):116. doi: 10.1186/s13244-025-01993-9. Insights Imaging. 2025. PMID: 40464876 Free PMC article.
-
Applicability and potential of monitored reconstruction in computed tomography.PLoS One. 2024 Jul 22;19(7):e0307231. doi: 10.1371/journal.pone.0307231. eCollection 2024. PLoS One. 2024. PMID: 39037982 Free PMC article.
References
-
- Innocenti F, Del Taglia B, Tassinari I, Trausi F, Conti A, Zanobetti M, et al.. Utility of repeat head computed tomography after mild head trauma: influence on short- and long-term prognosis and health-related quality of life. Intern Emerg Med. 2017;12(1):81–9. doi: 10.1007/s11739-016-1421-y - DOI - PubMed
-
- Karami V, Albosof M, Najarian M, Gholami M. Assessment of Commercially Available In-plane Bismuth Breast Shields for Clinical Use in Patients Undergoing Thoracic Computed Tomography. Hong Kong J Radiol. 2021;24:108–15.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
