

Virological Failure After Switch to Long-Acting Cabotegravir and Rilpivirine Injectable Therapy: An In-depth Analysis
- PMID: 38207125
- PMCID: PMC11259215
- DOI: 10.1093/cid/ciae016
Virological Failure After Switch to Long-Acting Cabotegravir and Rilpivirine Injectable Therapy: An In-depth Analysis
Abstract
Background: Long-acting (LA) injectable therapy with cabotegravir (CAB) and rilpivirine (RPV) is currently used as maintenance treatment for human immunodeficiency virus type 1, and has a low risk for virological failure (VF). Although the risk is low, the circumstances and impact of VF in the real-world setting merit further evaluation.
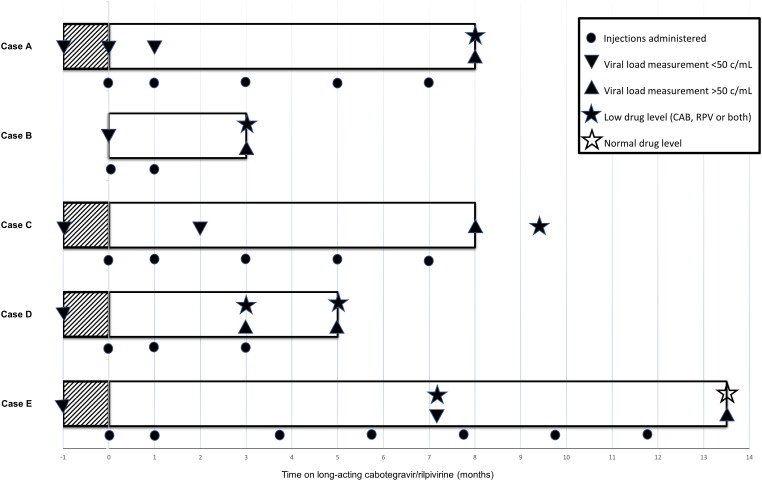
Methods: We performed an in-depth clinical, virological, and pharmacokinetic analysis on the reasons behind and the impact of VF during LA CAB/RPV therapy in 5 cases from the Netherlands. Genotypic resistance testing was performed after the occurrence of VF, and drug plasma (trough) concentrations were measured after VF was established and on any other samples to assess on-treatment drug levels. CAB and RPV drug levels that were below the first quartile of the population cutoff (≤Q1) were considered to be low.
Results: Five cases who were eligible for LA CAB/RPV experienced VF despite a low predicted risk at baseline. Genotypic resistance testing revealed extensive selection of nonnucleoside reverse transcriptase inhibitor-associated mutations in all cases, and integrase strand transfer inhibitor mutations in 4 cases. All cases displayed low drug levels of either CAB, RPV, or both during the treatment course, likely contributing to the occurrence of VF. In 3 cases, we were able to identify the potential mechanisms behind these low drug levels.
Conclusions: This is the first in-depth multiple case analysis of VF on LA CAB/RPV therapy in a real-world setting. Our observations stress the need to be aware for (evolving) risk factors and the yield of a comprehensive clinical, virological, and pharmacokinetic approach in case of failure.
Keywords: cabotegravir; injectables; long-acting; rilpivirine; virological failure.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. B. J. W. received a research grant from Gilead Health Sciences as well as speaker’s and advisory board fees from Gilead Health Sciences and ViiV Healthcare; all fees were paid to institution. J. H. G. reports participation as a speaker for the Masterclass Infectieziekten in the Netherlands, as well as President of Dutch Society of HIV treating physicians. M. V. received grants and consultancy fees from ViiV Healthcare, Gilead Health Sciences, and MSD, all paid to institution. D. B. received a research grant and honoraria for lectures from ViiV Healthcare. A. M. J. W. received investigator-initiated research grants from Gilead Sciences, AIDSfonds, and Nederlandse organisatie voor Wetenschappelijk Onderzoek; support for attending the Virology Education conference from the European AIDS Clinical Society; receipt of drug level kits from ARK, and consultancy fees from ViiV Healthcare/GSK and Gilead Sciences, all paid to institution; Member of the board of the European Society for Translational Antiviral Research and Chair of the IAS-USA resistance mutation group, all unpaid. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- European Medicines Agency . First long-acting injectable antiretroviral therapy for HIV recommended for approval. 2020. Available at: https://www.ema.europa.eu/en/news/first-long-acting-injectable-antiretro.... Accessed 27 October 2023.
-
- Ambrosioni J, Levi L, Alagaratnam J, et al. Major revision version 12.0 of the European AIDS Clinical Society guidelines 2023. HIV Med 2023; 24:1126–36. - PubMed
-
- Gandhi RT, Bedimo R, Hoy JF, et al. Antiretroviral drugs for treatment and prevention of HIV infection in adults: 2022 recommendations of the International Antiviral Society–USA panel. JAMA 2023; 329:63–84. - PubMed
-
- Orkin C, Arasteh K, Górgolas Hernández-Mora M, et al. Long-acting cabotegravir and rilpivirine after oral induction for HIV-1 infection. N Engl J Med 2020; 382:1124–35. - PubMed
-
- Orkin C, Bernal Morell E, Tan DHS, et al. Initiation of long-acting cabotegravir plus rilpivirine as direct-to-injection or with an oral lead-in in adults with HIV-1 infection: week 124 results of the open-label phase 3 FLAIR study. Lancet HIV 2021; 8:e668–78. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
