

Impact of opioid-free analgesia on pain severity and patient satisfaction after discharge from surgery: multispecialty, prospective cohort study in 25 countries
- PMID: 38207169
- PMCID: PMC10783642
- DOI: 10.1093/bjs/znad421
Impact of opioid-free analgesia on pain severity and patient satisfaction after discharge from surgery: multispecialty, prospective cohort study in 25 countries
Erratum in
-
Corrigendum to: Impact of opioid-free analgesia on pain severity and patient satisfaction after discharge from surgery: multispecialty, prospective cohort study in 25 countries.Br J Surg. 2024 Jun 12;111(6):znae152. doi: 10.1093/bjs/znae152. Br J Surg. 2024. PMID: 38915254 Free PMC article. No abstract available.
Abstract
Background: Balancing opioid stewardship and the need for adequate analgesia following discharge after surgery is challenging. This study aimed to compare the outcomes for patients discharged with opioid versus opioid-free analgesia after common surgical procedures.
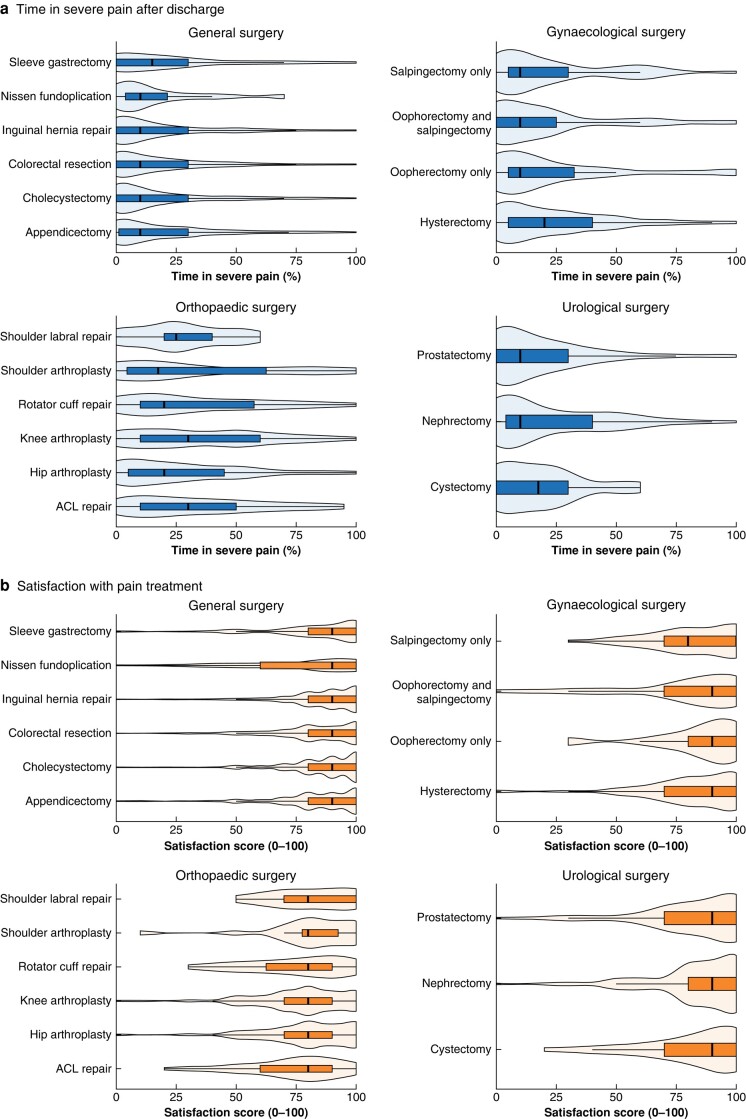
Methods: This international, multicentre, prospective cohort study collected data from patients undergoing common acute and elective general surgical, urological, gynaecological, and orthopaedic procedures. The primary outcomes were patient-reported time in severe pain measured on a numerical analogue scale from 0 to 100% and patient-reported satisfaction with pain relief during the first week following discharge. Data were collected by in-hospital chart review and patient telephone interview 1 week after discharge.
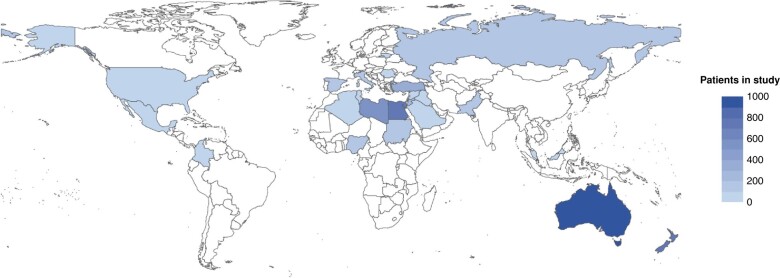
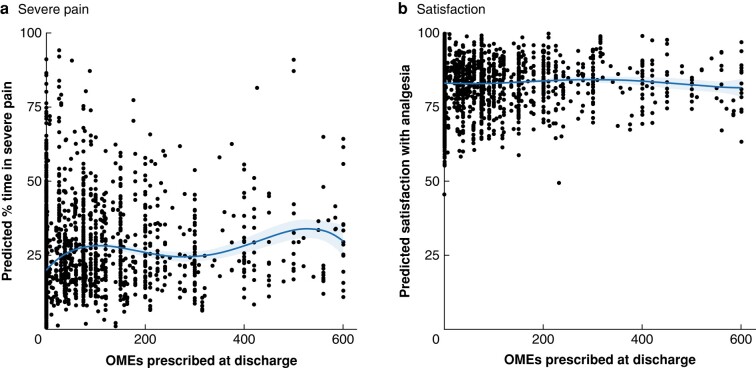
Results: The study recruited 4273 patients from 144 centres in 25 countries; 1311 patients (30.7%) were prescribed opioid analgesia at discharge. Patients reported being in severe pain for 10 (i.q.r. 1-30)% of the first week after discharge and rated satisfaction with analgesia as 90 (i.q.r. 80-100) of 100. After adjustment for confounders, opioid analgesia on discharge was independently associated with increased pain severity (risk ratio 1.52, 95% c.i. 1.31 to 1.76; P < 0.001) and re-presentation to healthcare providers owing to side-effects of medication (OR 2.38, 95% c.i. 1.36 to 4.17; P = 0.004), but not with satisfaction with analgesia (β coefficient 0.92, 95% c.i. -1.52 to 3.36; P = 0.468) compared with opioid-free analgesia. Although opioid prescribing varied greatly between high-income and low- and middle-income countries, patient-reported outcomes did not.
Conclusion: Opioid analgesia prescription on surgical discharge is associated with a higher risk of re-presentation owing to side-effects of medication and increased patient-reported pain, but not with changes in patient-reported satisfaction. Opioid-free discharge analgesia should be adopted routinely.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gan TJ, Habib AS, Miller TE, White W, Apfelbaum JL. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin 2014;30:149–160 - PubMed
-
- Macintyre PE, Quinlan J, Levy N, Lobo DN. Current issues in the use of opioids for the management of postoperative pain: a review. JAMA Surg 2022;157:158–166 - PubMed
-
- The Lancet Public Health . Opioid overdose crisis: time for a radical rethink. Lancet Public Health 2022;7:e195. - PubMed
-
- Oderda GM, Said Q, Evans RS, Stoddard GJ, Lloyd J, Jackson Ket al. . Opioid-related adverse drug events in surgical hospitalizations: impact on costs and length of stay. Ann Pharmacother 2007;41:400–406 - PubMed
