

MYC rearrangements in HIV-associated large B-cell lymphomas: EUROMYC, a European retrospective study
- PMID: 38207206
- PMCID: PMC10877133
- DOI: 10.1182/bloodadvances.2023010704
MYC rearrangements in HIV-associated large B-cell lymphomas: EUROMYC, a European retrospective study
Abstract
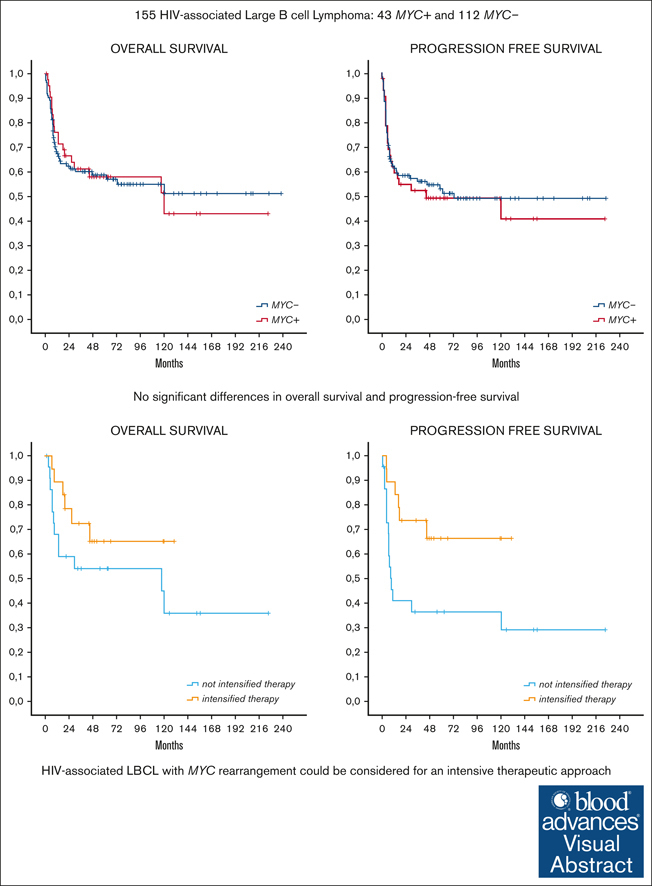
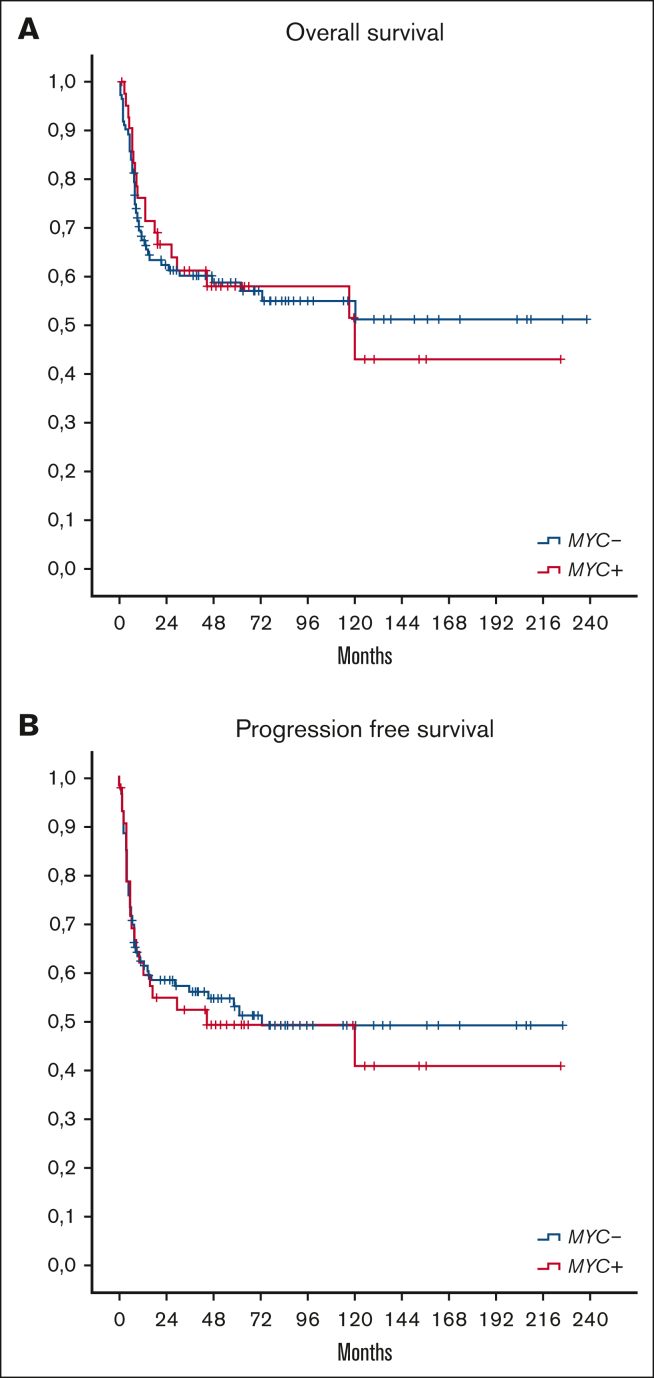
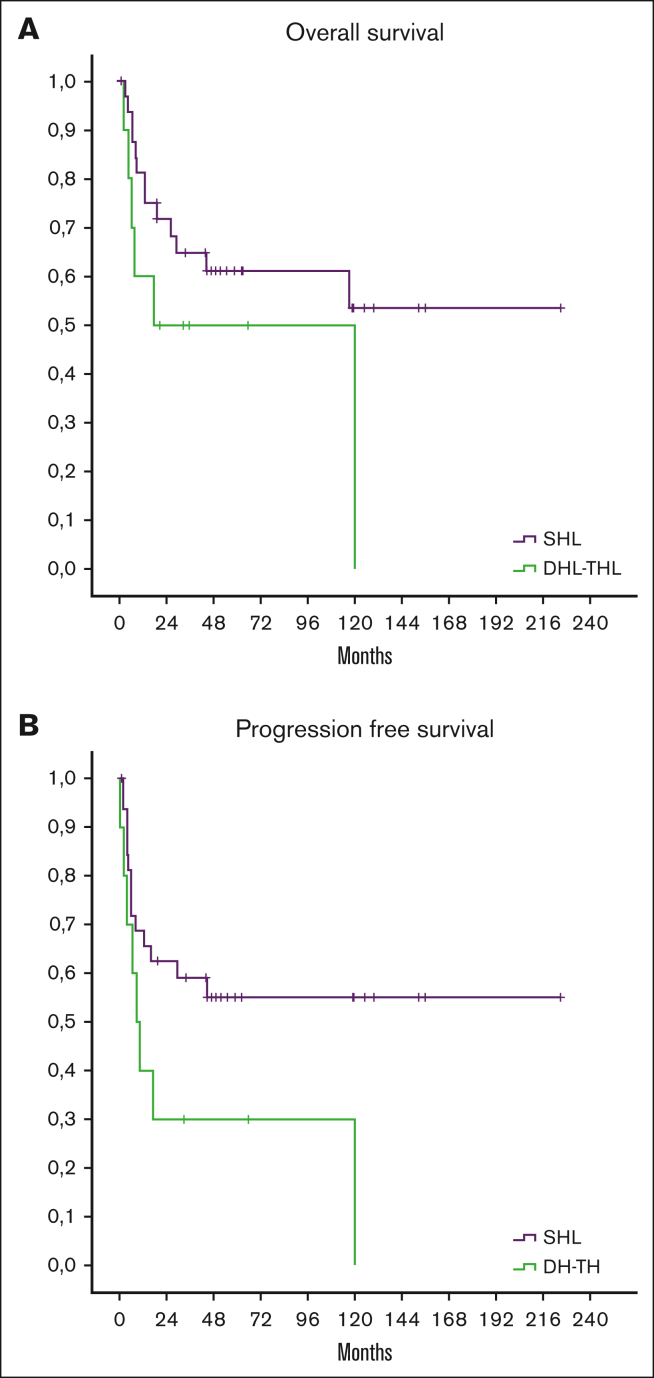
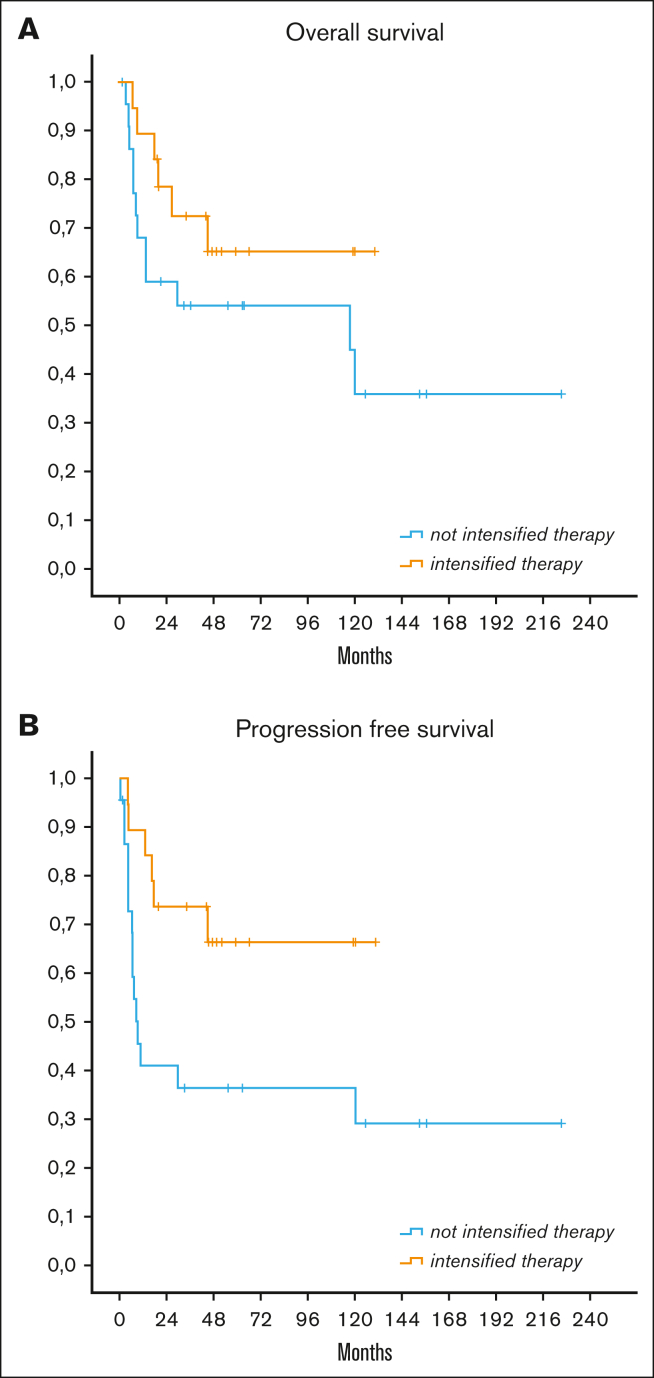
Large B-cell lymphoma (LBCL) carrying MYC rearrangement, alone or together with BCL2 and/or BCL6 translocations, have shown a poor prognosis when treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) in the HIV population. Scanty data are available on the prevalence and prognostic impact of MYC rearrangements in HIV-associated LBCL. We conducted a retrospective study to evaluate the clinical effect of MYC rearrangement in HIV-associated LBCL. We evaluated clinical characteristics, treatment received, and outcome of LBCL in patients with HIV with MYC rearrangement (MYC+) and without MYC rearrangement (MYC-). A total of 155 patients with HIV who had received fluorescence in situ hybridization analysis for MYC were enrolled in 11 European centers: 43 with MYC+ and 112 MYC-. Among patients with MYC, 10 had double-/triple-hit lymphomas, and 33 had isolated MYC rearrangement (single-hit lymphoma). Patients with MYC+ had more frequently advanced stage, >2 extranodal site at presentation, and higher proliferative index. There were no significant differences in overall survival and progression-free survival (PFS) between the 2 groups. However, patients with MYC+ received more frequently intensive chemotherapy (iCT) (44%) than (R)CHOP alone (35%) or infusional treatment (DA-EPOCH-R and R-CDE) (19%). Among patients with MYC+, those who received iCT achieved a better outcome than patients who received nonintensive treatment (complete remission, 84% vs 52%; P = .028; 5-year PFS, 66% vs 36%; P = .021). Our retrospective results suggest that HIV-associated LBCL with MYC+ could be considered for an intensive therapeutic approach whenever possible, whereas (R)CHOP seems to give inferior results in this subset of patients in terms of complete remission and PFS.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: M.S. reports honoraria from Gilead, Servier, Novartis, Incyte, BeiGene, and Istituto Gentili; and research funding from Menarini. L.A. reports consultancy fees from or advisory role in Roche, Janssen-Cilag, Verastem, Incyte, EUSA Pharma, Celgene/Bristol Myers Squibb, Kite/Gilead, and ADC Therapeutics; speakers’ bureau fees from EUSA Pharma and Novartis; and research funding from Gilead Sciences. D.D. reports travel grants from Roche, Gentili, Lilly, and Eisai; and other remuneration from Gentili and Daikii Sanchio. The remaining authors declare no competing financial interests.
Figures
References
-
- Swerdlow SH, Campo E, Harris NL, et al. IARC Press; 2017. WHO classification of tumors of Haematopoietic and Lymphoid Tissues.
-
- Landsburg DJ, Nasta SD, Svoboda J, Morrissette JJ, Schuster SJ. 'Double-Hit' cytogenetic status may not be predicted by baseline clinicopathological characteristics and is highly associated with overall survival in B cell lymphoma patients. Br J Haematol. 2014;166(3):369–374. - PubMed
-
- Li S, Desai P, Lin P, et al. MYC/BCL6 double-hit lymphoma (DHL): a tumour associated with an aggressive clinical course and poor prognosis. Histopatology. 2016;68(7):1090–1098. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
