

Brief Assessment of Patient Phenotype to Explain Variability in Postsurgical Pain and Opioid Consumption after Cesarean Delivery: Performance of a Novel Brief Questionnaire Compared to Long Questionnaires
- PMID: 38207329
- PMCID: PMC10939890
- DOI: 10.1097/ALN.0000000000004900
Brief Assessment of Patient Phenotype to Explain Variability in Postsurgical Pain and Opioid Consumption after Cesarean Delivery: Performance of a Novel Brief Questionnaire Compared to Long Questionnaires
Abstract
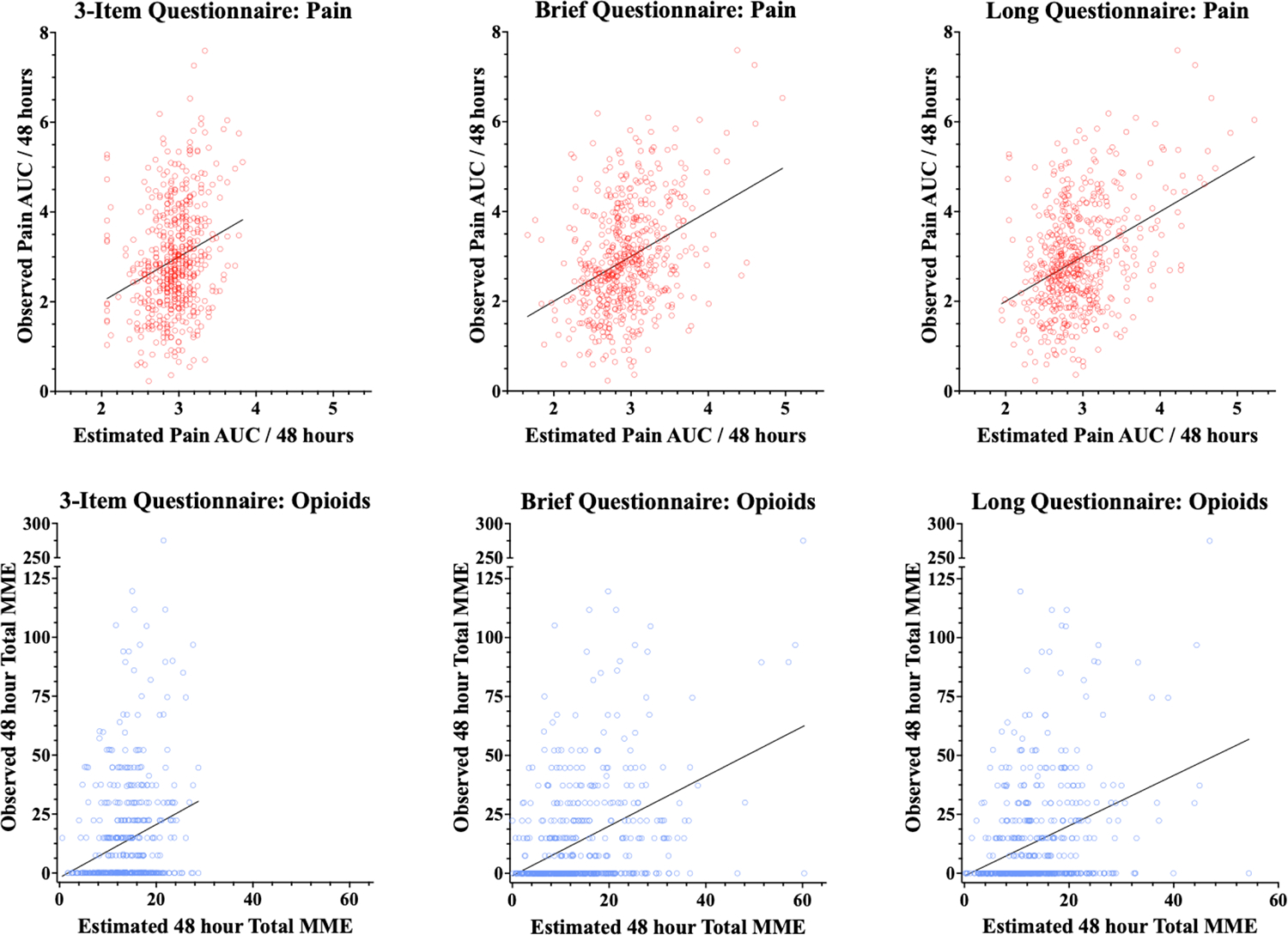
Background: Understanding factors that explain why some women experience greater postoperative pain and consume more opioids after cesarean delivery is crucial to building an evidence base for personalized prevention. Comprehensive psychosocial assessment with validated questionnaires in the preoperative period can be time-consuming. A three-item questionnaire has shown promise as a simpler tool to be integrated into clinical practice, but its brevity may limit the ability to explain heterogeneity in psychosocial pain modulators among individuals. This study compared the explanatory ability of three models: (1) the 3-item questionnaire, (2) a 58-item questionnaire (long) including validated questionnaires (e.g., Brief Pain Inventory, Patient Reported Outcome Measurement Information System [PROMIS]) plus the 3-item questionnaire, and (3) a novel 19-item questionnaire (brief) assessing several psychosocial factors plus the 3-item questionnaire. Additionally, this study explored the utility of adding a pragmatic quantitative sensory test to models.
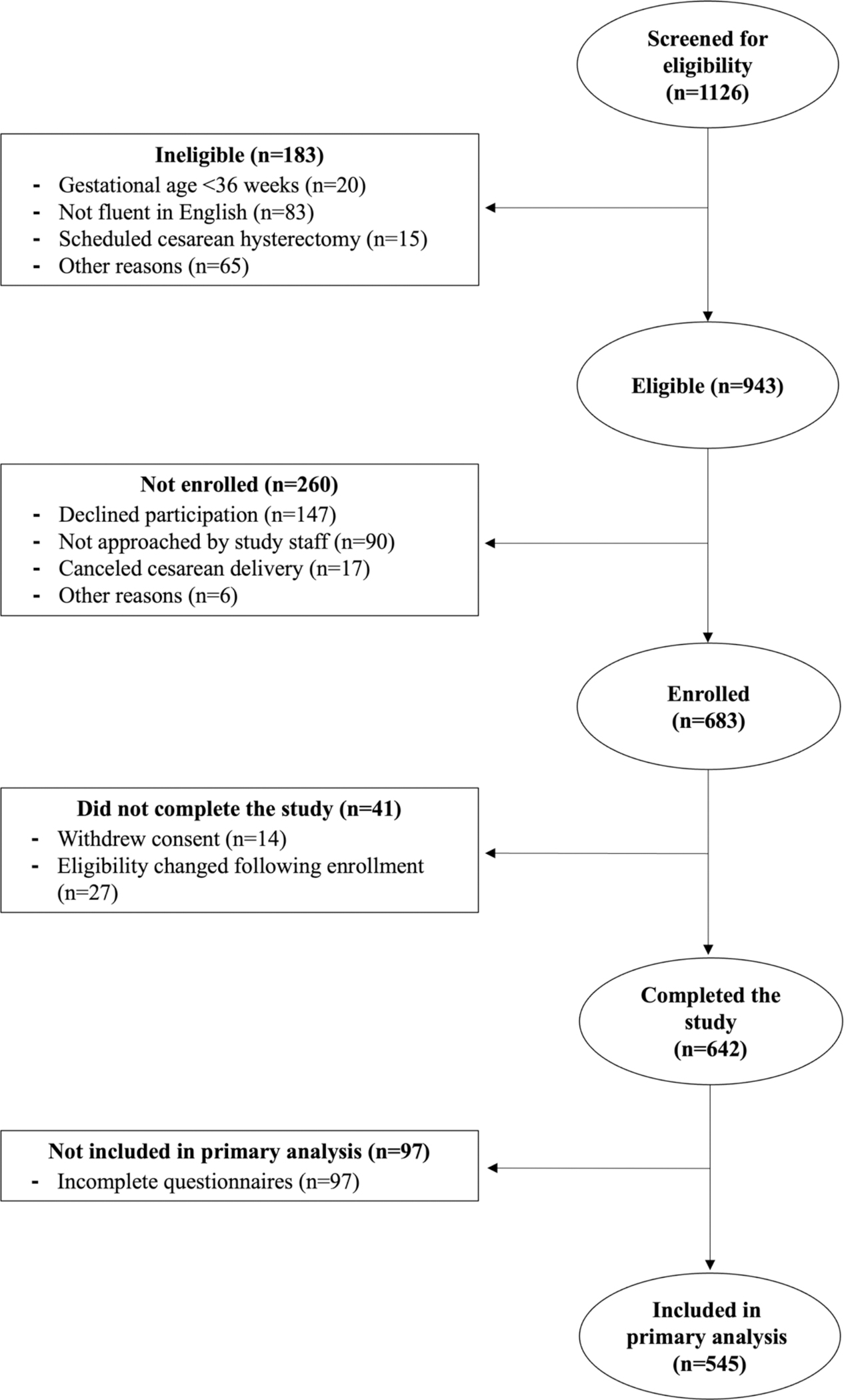
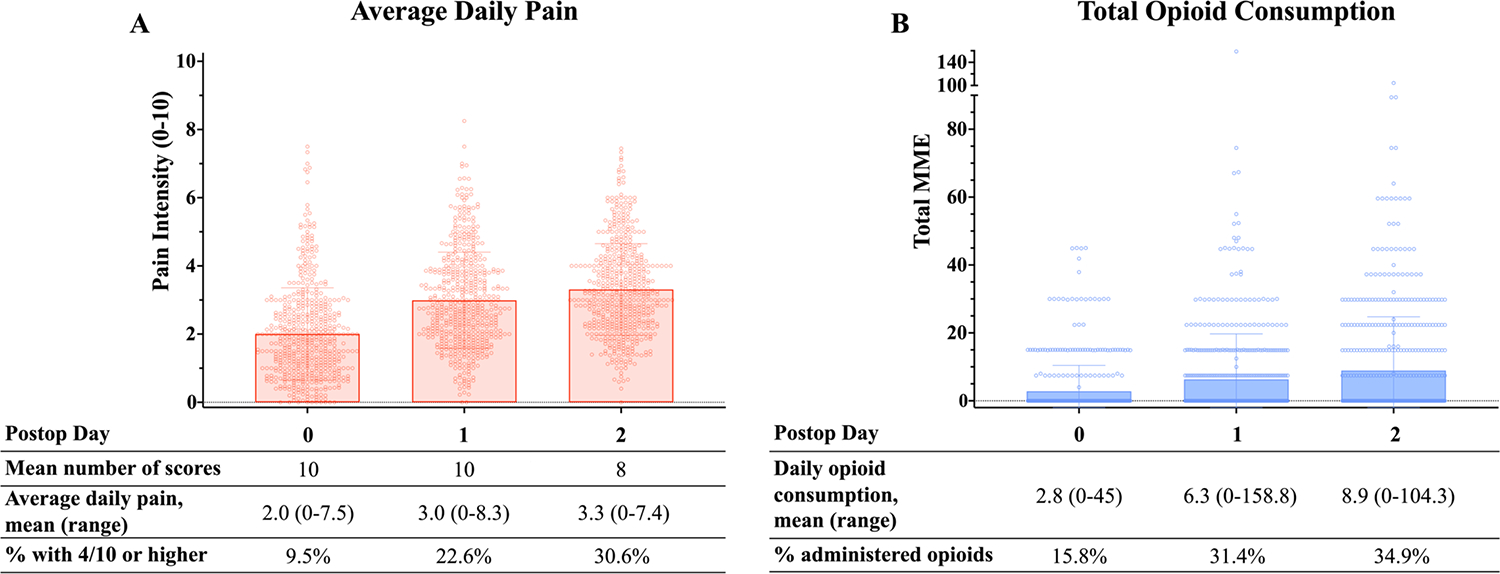
Methods: In this prospective, observational study, 545 women undergoing cesarean delivery completed questionnaires presurgery. Pain during local anesthetic skin wheal before spinal placement served as a pragmatic quantitative sensory test. Postoperatively, pain and opioid consumption were assessed. Linear regression analysis assessed model fit and the association of model items with pain and opioid consumption during the 48 h after surgery.
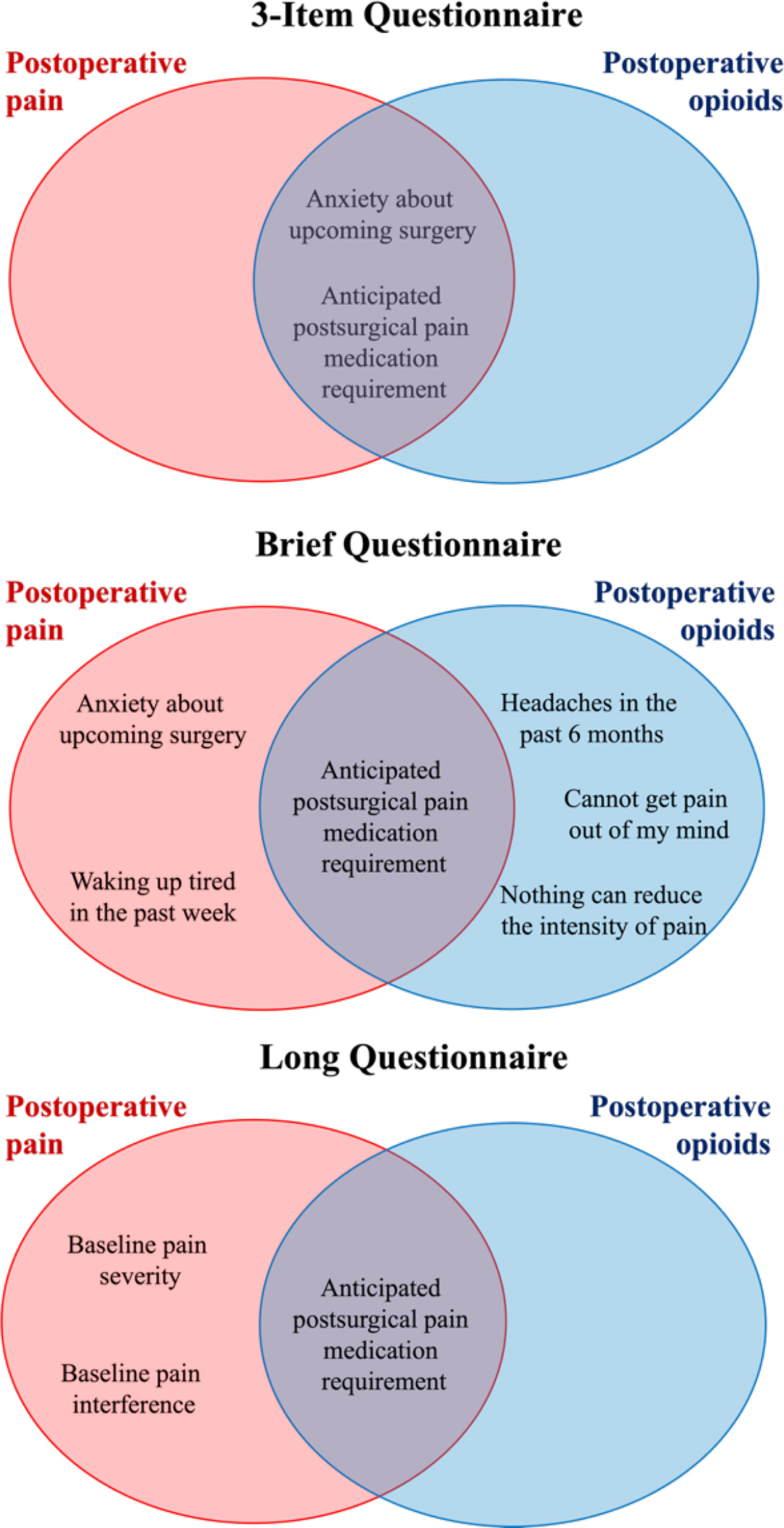
Results: A modest amount of variability was explained by each of the three models for postoperative pain and opioid consumption. Both the brief and long questionnaire models performed better than the three-item questionnaire but were themselves statistically indistinguishable. Items that were independently associated with pain and opioid consumption included anticipated postsurgical pain medication requirement, surgical anxiety, poor sleep, pre-existing pain, and catastrophic thinking about pain. The quantitative sensory test was itself independently associated with pain across models but only modestly improved models for postoperative pain.
Conclusions: The brief questionnaire may be more clinically feasible than longer validated questionnaires, while still performing better and integrating a more comprehensive psychosocial assessment than the three-item questionnaire.
Copyright © 2024 American Society of Anesthesiologists. All Rights Reserved.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
