

Fc receptor-like 5 (FCRL5)-directed CAR-T cells exhibit antitumor activity against multiple myeloma
- PMID: 38212320
- PMCID: PMC10784595
- DOI: 10.1038/s41392-023-01702-2
Fc receptor-like 5 (FCRL5)-directed CAR-T cells exhibit antitumor activity against multiple myeloma
Abstract
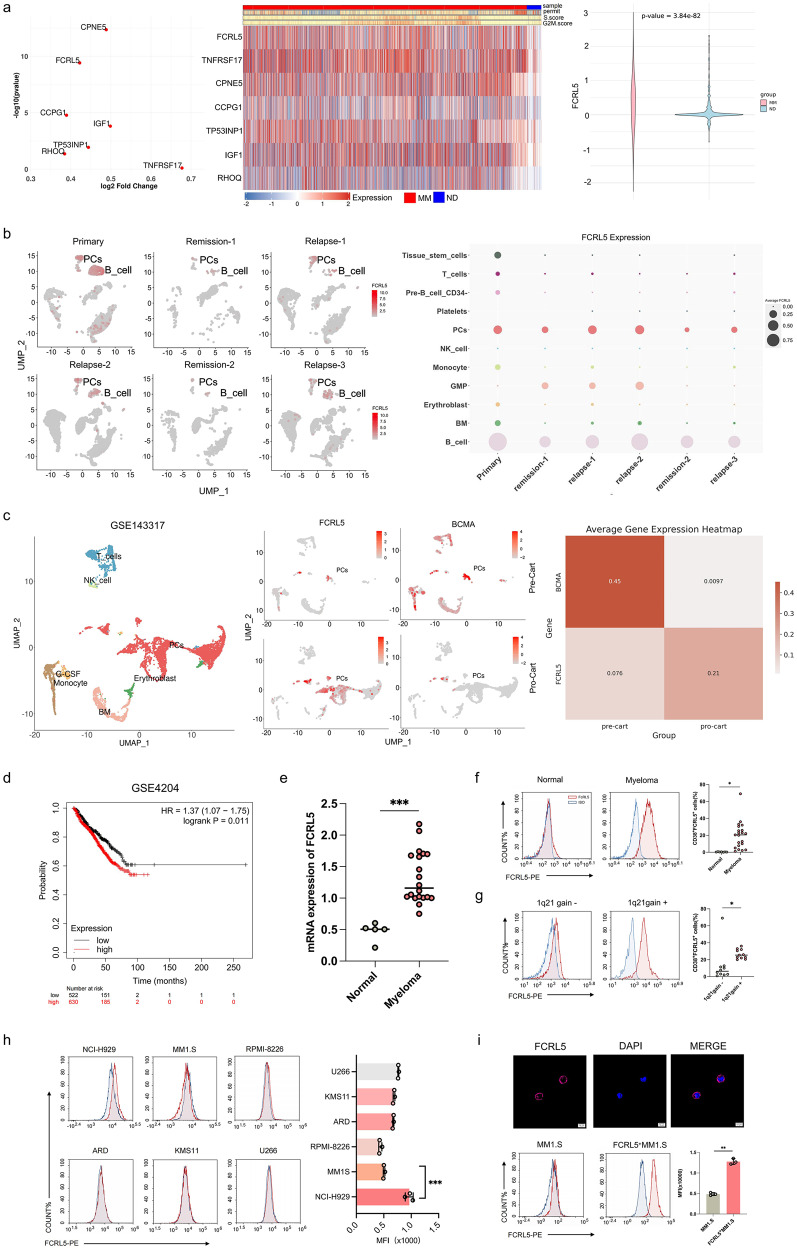
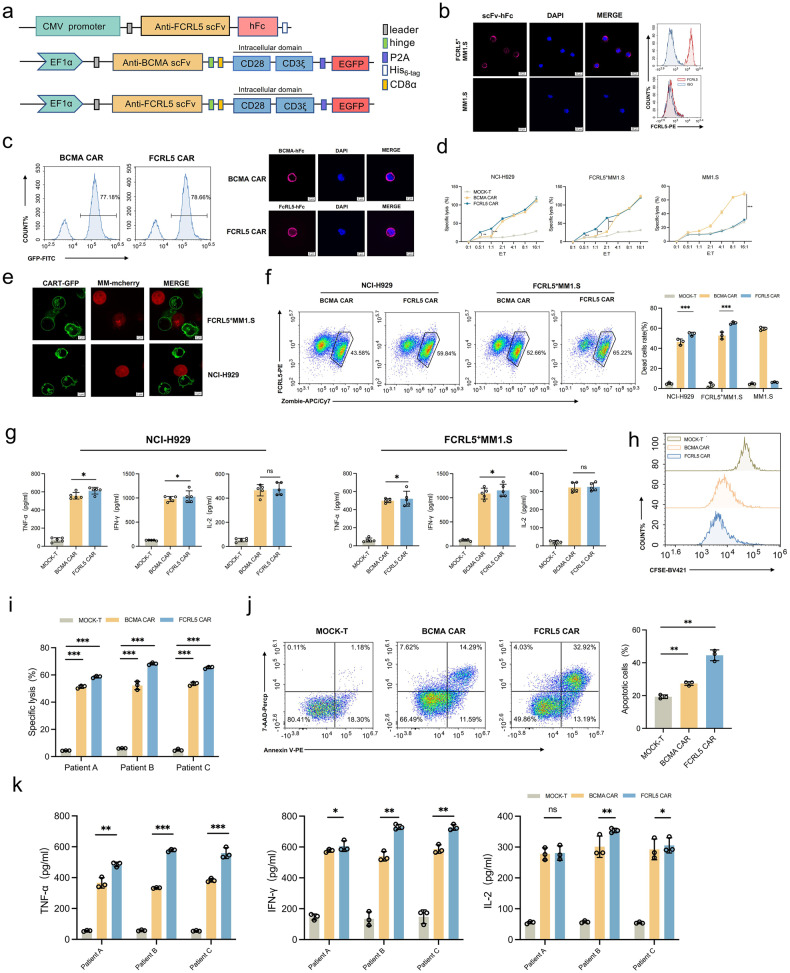
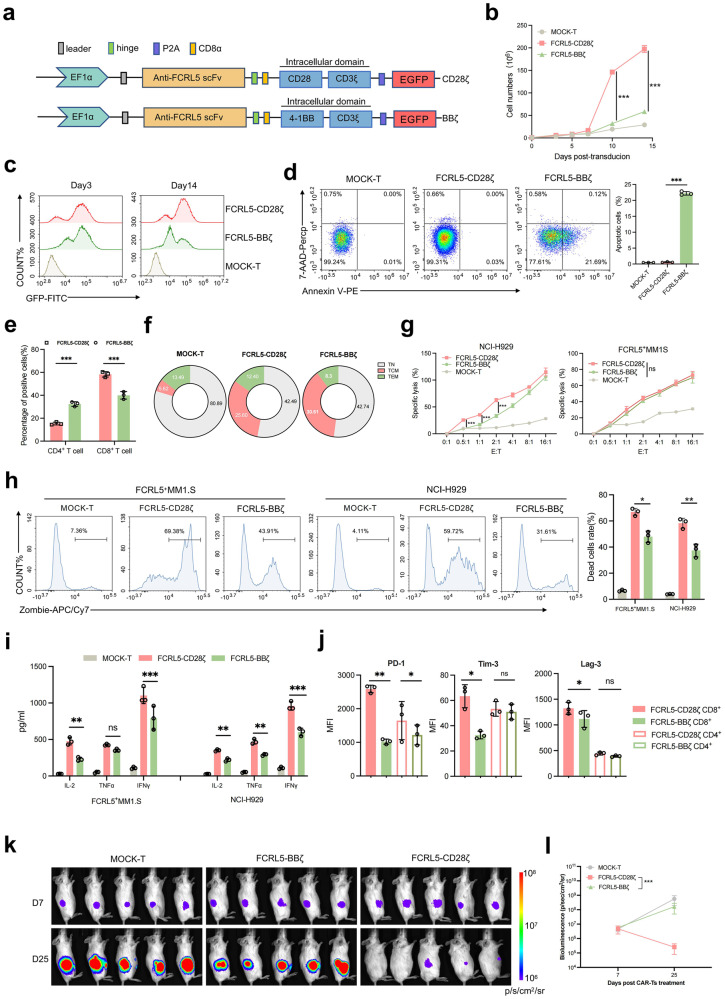
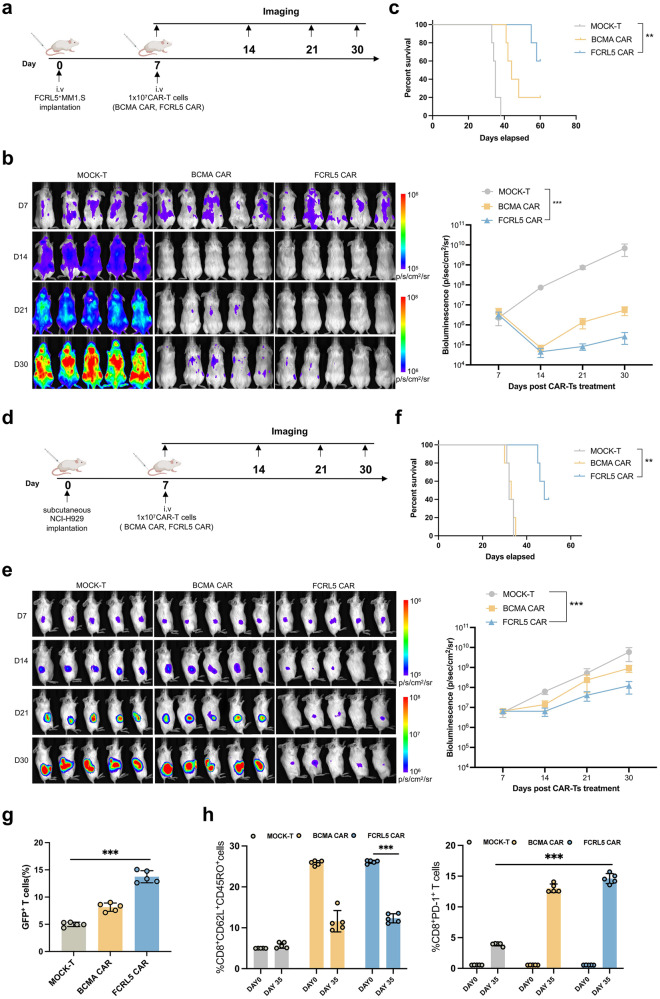
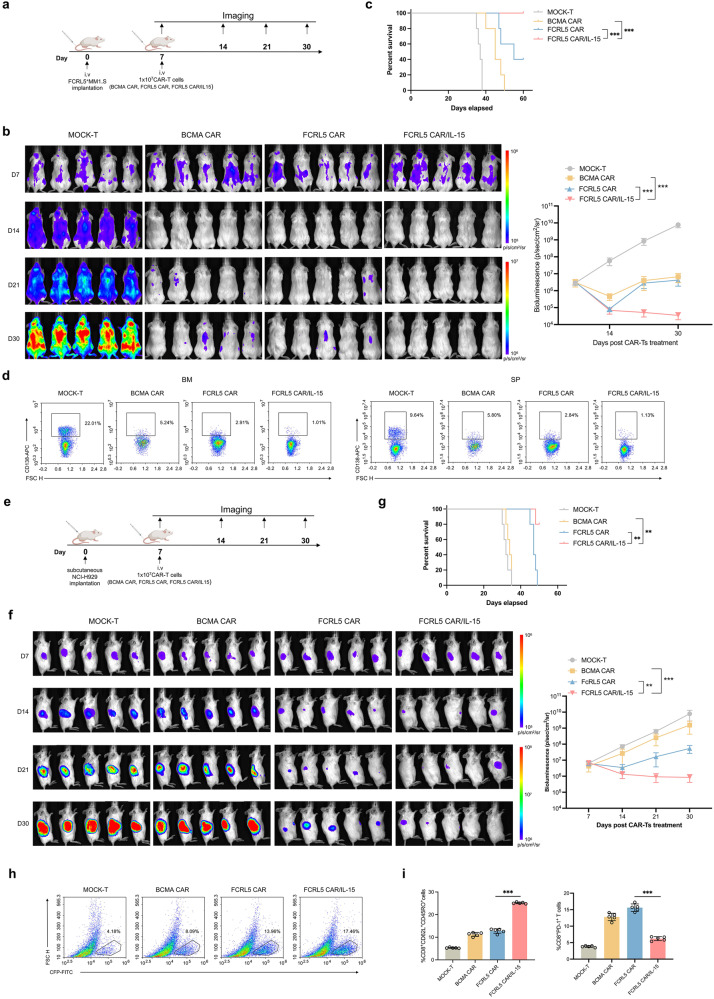
Multiple myeloma (MM) remains a challenging hematologic malignancy despite advancements in chimeric antigen receptor T-cell (CAR-T) therapy. Current targets of CAR-T cells used in MM immunotherapy have limitations, with a subset of patients experiencing antigen loss resulting in relapse. Therefore, novel targets for enhancing CAR-T cell therapy in MM remain needed. Fc receptor-like 5 (FCRL5) is a protein marker with considerably upregulated expression in MM and has emerged as a promising target for CAR-T cell therapeutic interventions, offering an alternative treatment for MM. To further explore this option, we designed FCRL5-directed CAR-T cells and assessed their cytotoxicity in vitro using a co-culture system and in vivo using MM cell-derived xenograft models, specifically focusing on MM with gain of chromosome 1q21. Given the challenges in CAR-T therapies arising from limited T cell persistence, our approach incorporates interleukin-15 (IL-15), which enhances the functionality of central memory T (TCM) cells, into the design of FCRL5-directed CAR-T cells, to improve cytotoxicity and reduce T-cell dysfunction, thereby promoting greater CAR-T cell survival and efficacy. Both in vitro and xenograft models displayed that FCRL5 CAR-T cells incorporating IL-15 exhibited potent antitumor efficacy, effectively inhibiting the proliferation of MM cells and leading to remarkable tumor suppression. Our results highlight the capacity of FCRL5-specific CAR-T cells with the integration of IL-15 to improve the therapeutic potency, suggesting a potential novel immunotherapeutic strategy for MM treatment.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
